

Longitudinal tracking of left atrial diameter over the adult life course: Clinical correlates in the community
- PMID: 20100973
- PMCID: PMC2823068
- DOI: 10.1161/CIRCULATIONAHA.109.885806
Longitudinal tracking of left atrial diameter over the adult life course: Clinical correlates in the community
Abstract
Background: Increased left atrial diameter (LAD) is associated with elevated risk of atrial fibrillation (AF) and cardiovascular disease. Information is limited regarding the short- or long-term correlates of LAD.
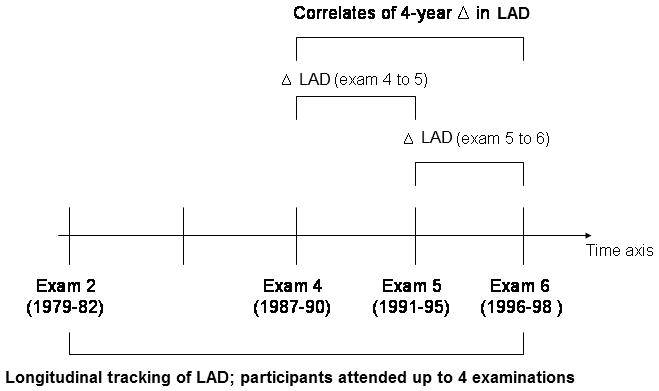
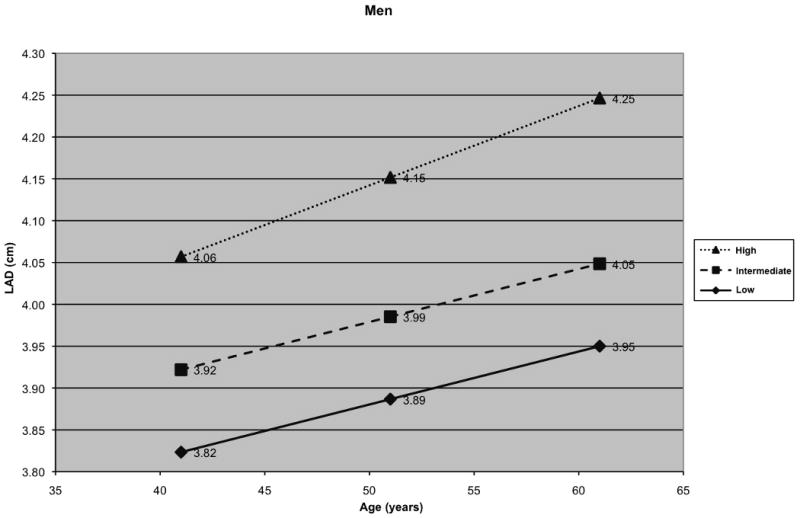
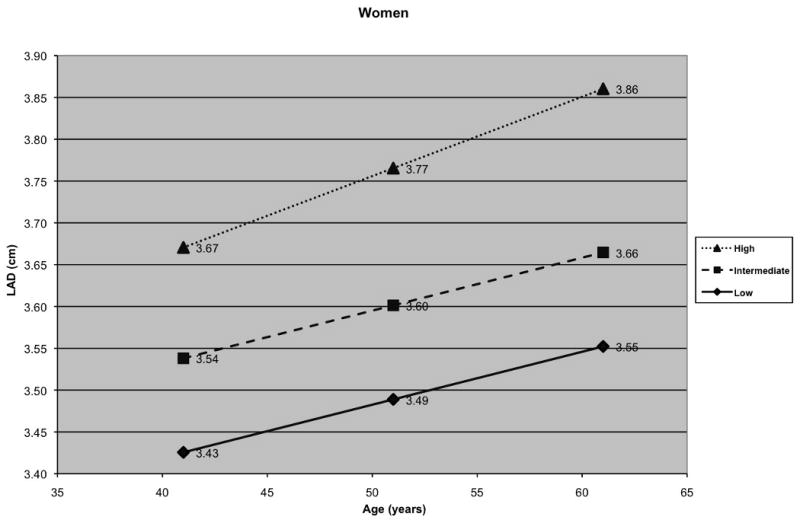
Methods and results: We evaluated clinical correlates of LAD for a 16-year period in 4403 Framingham Study participants (mean age, 45 years; 52% women; median observations/participant=3) using multilevel modeling. We related age, sex, body mass index (BMI), systolic and diastolic blood pressure (BP), diabetes, and antihypertensive treatment to LAD. Sex-specific growth curves for LAD were estimated for individuals with low, intermediate, and high risk factor burden. We also related risk factors to changes in LAD during a 4-year period in 3365 participants. Age, male sex (3.83 mm compared to women), greater BMI, higher systolic BP (0.24 mm per 10 mm Hg increment), and antihypertensive treatment (0.54 mm) were associated positively with LAD (P<0.001). Men had a greater increase in LAD with BMI than women (2.02 versus 1.77 mm in women, per 5-unit increment), and individuals receiving antihypertensive treatment experienced a greater increase in LAD with age (0.95 versus 0.63 mm per 10-year age increment) when compared with those not receiving antihypertensive treatment. Overall, greater risk factor burden was positively associated with LAD. These risk factors were also associated positively with 4-year change in LAD (P<0.001).
Conclusions: Our longitudinal study of a large community-based sample identified higher BP and greater BMI as key modifiable correlates of LAD, suggesting that maintaining optimal levels of these risk factors through the life course may prevent atrial remodeling and AF.
Conflict of interest statement
Figures
References
-
- Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, Singer DE. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285:2370–2375. - PubMed
-
- Benjamin EJ, Chen PS, Bild DE, Mascette AM, Albert CM, Alonso A, Calkins H, Connolly SJ, Curtis AB, Darbar D, Ellinor PT, Go AS, Goldschlager NF, Heckbert SR, Jalife J, Kerr CR, Levy D, Lloyd-Jones DM, Massie BM, Nattel S, Olgin JE, Packer DL, Po SS, Tsang TS, Van Wagoner DR, Waldo AL, Wyse DG. Prevention of atrial fibrillation: report from a national heart, lung, and blood institute workshop. Circulation. 2009;119:606–618. - PMC - PubMed
-
- Vaziri SM, Larson MG, Benjamin EJ, Levy D. Echocardiographic predictors of nonrheumatic atrial fibrillation. The Framingham Heart Study. Circulation. 1994;89:724–730. - PubMed
-
- Benjamin EJ, D'Agostino RB, Belanger AJ, Wolf PA, Levy D. Left atrial size and the risk of stroke and death. The Framingham Heart Study. Circulation. 1995;92:835–841. - PubMed
-
- Laukkanen JA, Kurl S, Eranen J, Huttunen M, Salonen JT. Left atrium size and the risk of cardiovascular death in middle-aged men. Arch Intern Med. 2005;165:1788–1793. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01-HC-25195/HC/NHLBI NIH HHS/United States
- R01 NS017950/NS/NINDS NIH HHS/United States
- R01 HL092577/HL/NHLBI NIH HHS/United States
- N01 HC025195/HC/NHLBI NIH HHS/United States
- T32 HL007572/HL/NHLBI NIH HHS/United States
- K24 HL004334/HL/NHLBI NIH HHS/United States
- R01HL080124/HL/NHLBI NIH HHS/United States
- 6R01-NS 17950/NS/NINDS NIH HHS/United States
- R01 HL080124/HL/NHLBI NIH HHS/United States
- 1R01HL092577/HL/NHLBI NIH HHS/United States
- N01 HC025195/HL/NHLBI NIH HHS/United States
- 2 K24 HL04334/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
