

Structural integrity of corticospinal motor fibers predicts motor impairment in chronic stroke
- PMID: 20101033
- PMCID: PMC3122304
- DOI: 10.1212/WNL.0b013e3181ccc6d9
Structural integrity of corticospinal motor fibers predicts motor impairment in chronic stroke
Abstract
Objective: Motor impairment after stroke has been related to infarct size, infarct location, and integrity of motor tracts. To determine the value of diffusion tensor imaging (DTI) as a predictor of motor outcome and its role as a structural surrogate marker of impairment in chronic stroke, we tested correlations between motor impairment and DTI-derived measures of motor tract integrity.
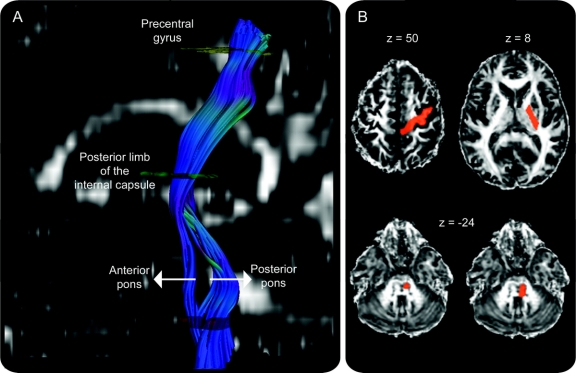
Methods: Thirty-five chronic stroke patients with varying degrees of recovery underwent DTI and motor impairment assessments. Fibers originating from the precentral gyrus were traced and separated into pyramidal tract (PT) and alternate motor fibers (aMF). Asymmetry indices of fiber number and regional fractional anisotropy (FA) values comparing lesional with nonlesional hemispheres were correlated with motor impairment scores and compared to an age-matched control group.
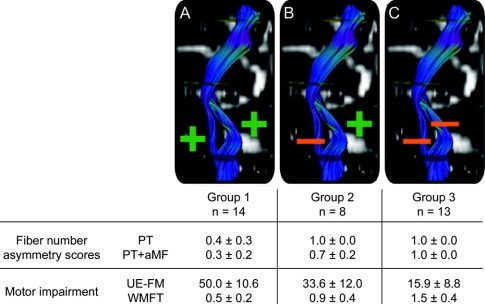
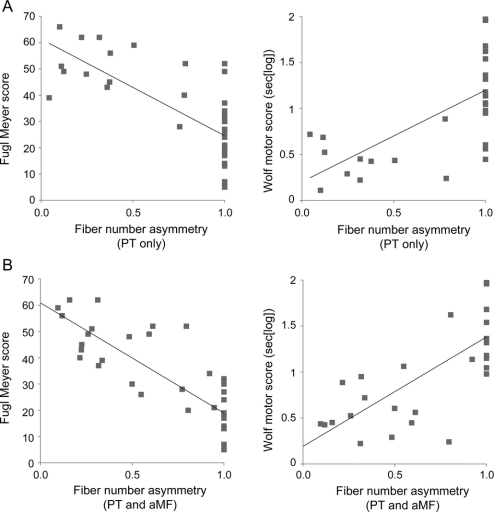
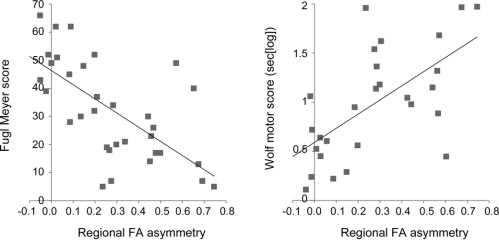
Results: Fiber number and regional FA value asymmetry significantly differed between the groups with lower values in the patients' lesional hemispheres. Both measures significantly predicted motor impairment with stronger predictions when all motor tracts were combined as compared to predictions using only the PT. The pattern of motor tract damage (PT only vs PT and aMF) led to a classification of mild, moderate, or severe impairment with significant between-group differences in motor impairment scores.
Conclusions: Diffusion tensor imaging-derived measures are valid structural markers of motor impairment. The integrity of all descending motor tracts, not merely the pyramidal tract, appears to account for stroke recovery. A 3-tier, hierarchical classification of impairment categories based on the pattern of motor tract damage is proposed that might be helpful in predicting recovery potential.
Figures
Comment in
-
Stroke recovery: the pyramid in focus.Neurology. 2010 Jan 26;74(4):276-7. doi: 10.1212/WNL.0b013e3181ccc758. Neurology. 2010. PMID: 20101032 No abstract available.
References
-
- Pineiro R, Pendlebury ST, Smith S, et al. Relating MRI changes to motor deficit after ischemic stroke by segmentation of functional motor pathways. Stroke 2000;31:672–679. - PubMed
-
- Schiemanck SK, Kwakkel G, Post MW, Kappelle LJ, Prevo AJ. Impact of internal capsule lesions on outcome of motor hand function at one year post-stroke. J Rehabil Med 2008;40:96–101. - PubMed
-
- Duncan PW. Stroke disability. Phys Ther 1994;74:399–407. - PubMed
-
- Cramer SC, Seitz RJ. Imaging functional recovery from stroke. In: Handbook of Clinical Neurology 2008;94:1097–1117. - PubMed
-
- Lang CE, Schieber MH. Human finger independence: limitations due to passive mechanical coupling versus active neuromuscular control. J Neurophysiol 2004;92:2802–2810. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 NS047029-04A2/NS/NINDS NIH HHS/United States
- 1P50 CA101942-01/CA/NCI NIH HHS/United States
- 1R01NS045049/NS/NINDS NIH HHS/United States
- 1R01 DC008796/DC/NIDCD NIH HHS/United States
- 1R21 CA121570A1/CA/NCI NIH HHS/United States
- R01 DC009823-01/DC/NIDCD NIH HHS/United States
- R01-EB004582/EB/NIBIB NIH HHS/United States
- R01 NS045049/NS/NINDS NIH HHS/United States
- R01 MH80729-01A2/MH/NIMH NIH HHS/United States
- 1 R01 AG027435-01/AG/NIA NIH HHS/United States
- R01 DC008796/DC/NIDCD NIH HHS/United States
- 1 R01 CA115745-01A1/CA/NCI NIH HHS/United States
- R01DC008796-01A1/DC/NIDCD NIH HHS/United States
- R01 DC009823/DC/NIDCD NIH HHS/United States
- R01 MH077073-01A2/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical