

Accuracy of administrative databases in identifying patients with hypertension
- PMID: 20101286
- PMCID: PMC2801913
Accuracy of administrative databases in identifying patients with hypertension
Abstract
Background: Traditionally, the determination of the occurrence of hypertension in patients has relied on costly and time-consuming survey methods that do not allow patients to be followed over time.
Objectives: To determine the accuracy of using administrative claims data to identify rates of hypertension in a large population living in a single-payer health care system.
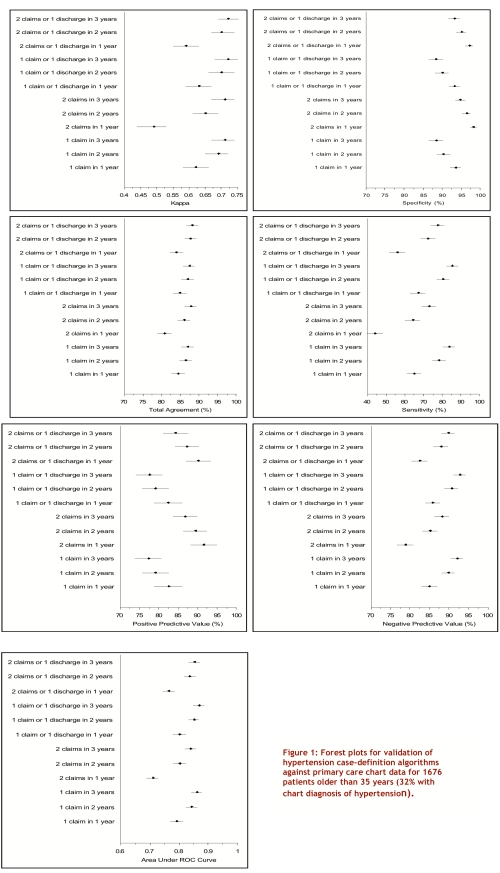
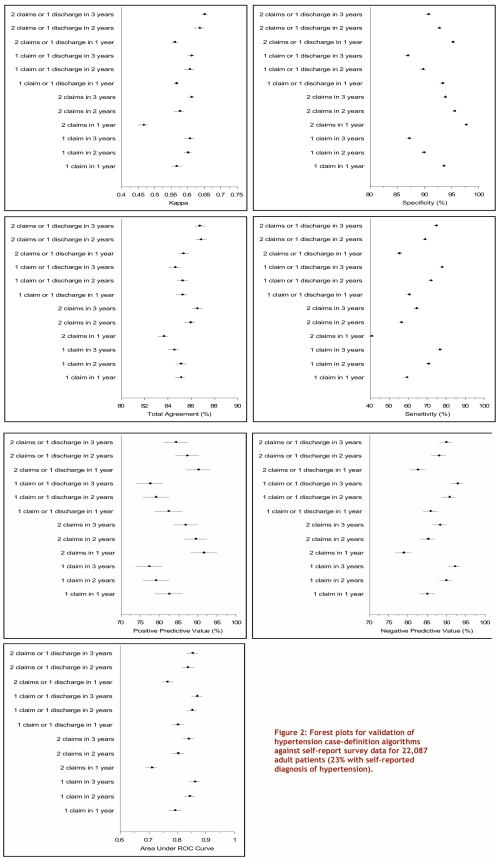
Methods: Various definitions for hypertension using administrative claims databases were compared with 2 other reference standards: (1) data obtained from a random sample of primary care physician offices throughout the province, and (2) self-reported survey data from a national census.
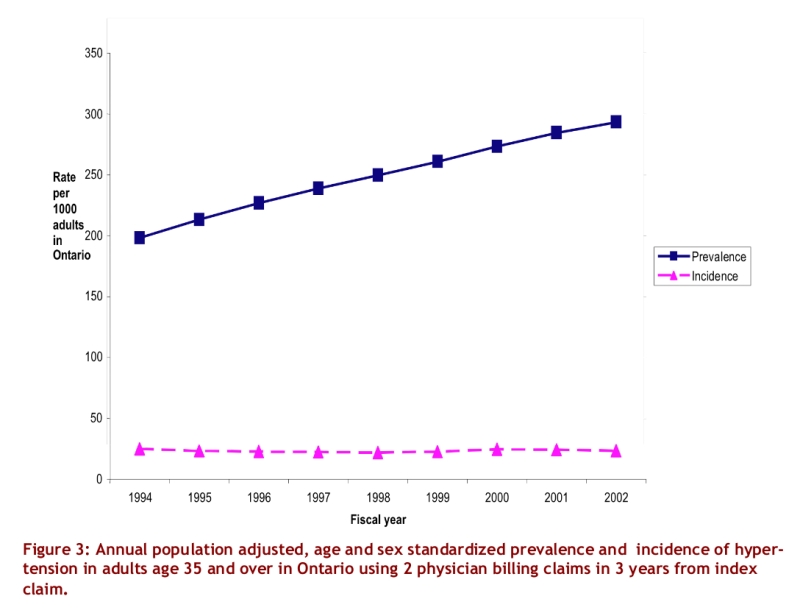
Results: A case-definition algorithm employing 2 outpatient physician billing claims for hypertension over a 3-year period had a sensitivity of 73% (95% confidence interval [CI] 69%-77%), a specificity of 95% (CI 93%-96%), a positive predictive value of 87% (CI 84%-90%), and a negative predictive value of 88% (CI 86%-90%) for detecting hypertensive adults compared with physician-assigned diagnoses. Compared with self-reported survey data, the algorithm had a sensitivity of 64% (CI 63%-66%), a specificity of 94%(CI 93%-94%), a positive predictive value of 77% (76%-78%), and negative predictive value of 89% (CI 88%-89%). When this algorithm was applied to the entire province of Ontario, the age- and sex-standardized prevalence of hypertension in adults older than 35 years increased from 20% in 1994 to 29% in 2002.
Conclusions: It is possible to use administrative data to accurately identify from a population sample those patients who have been diagnosed with hypertension. Given that administrative data are already routinely collected, their use is likely to be substantially less expensive compared with serial cross-sectional or cohort studies for surveillance of hypertension occurrence and outcomes over time in a large population.
Conflict of interest statement
Competing interests: Dr. Campbell has been paid fees for speaking and for consulting by most pharmaceutical companies in Canada that produce prescription medications to lower blood pressure and has received research funds from Pfizer Canada, Sanofi-Aventis, Merck Frosst, Servier and Bristol-Myers-Squibb for research on the epidemiology of hypertension. Dr. Campbell also chairs the steering committee and executive committee of the Canadian Hypertension Education Program (CHEP) as a volunteer. CHEP has a mandate to improve the treatment and control of hypertension in Canada. Dr. McAlister has received operating grant funding from Pfizer Canada for an ongoing investigator-initiated trial co-funded by the Heart and Stroke Foundation of Canada and Pfizer Canada. The other authors have no potential conflicts of interest.
Figures
Similar articles
-
Is there value in using physician billing claims along with other administrative health care data to document the burden of adolescent injury? An exploratory investigation with comparison to self-reports in Ontario, Canada.BMC Health Serv Res. 2005 Feb 18;5(1):15. doi: 10.1186/1472-6963-5-15. BMC Health Serv Res. 2005. PMID: 15720709 Free PMC article.
-
Identification of Physician-Diagnosed Alzheimer's Disease and Related Dementias in Population-Based Administrative Data: A Validation Study Using Family Physicians' Electronic Medical Records.J Alzheimers Dis. 2016 Aug 10;54(1):337-49. doi: 10.3233/JAD-160105. J Alzheimers Dis. 2016. PMID: 27567819
-
Accuracy of Canadian health administrative databases in identifying patients with rheumatoid arthritis: a validation study using the medical records of rheumatologists.Arthritis Care Res (Hoboken). 2013 Oct;65(10):1582-91. doi: 10.1002/acr.22031. Arthritis Care Res (Hoboken). 2013. PMID: 23592598
-
Methods for systematic reviews of administrative database studies capturing health outcomes of interest.Vaccine. 2013 Dec 30;31 Suppl 10:K2-6. doi: 10.1016/j.vaccine.2013.06.048. Vaccine. 2013. PMID: 24331070 Review.
-
Estimating Disease Prevalence in Administrative Data.Clin Invest Med. 2022 Jun 26;45(2):E21-27. doi: 10.25011/cim.v45i2.38100. Clin Invest Med. 2022. PMID: 35752980 Review.
Cited by
-
Cardiovascular complications and mortality after diabetes diagnosis for South Asian and Chinese patients: a population-based cohort study.Diabetes Care. 2013 Sep;36(9):2670-6. doi: 10.2337/dc12-2105. Epub 2013 May 1. Diabetes Care. 2013. PMID: 23637350 Free PMC article.
-
Further validation that claims data are a useful tool for epidemiologic research on hypertension.BMC Public Health. 2013 Jan 18;13:51. doi: 10.1186/1471-2458-13-51. BMC Public Health. 2013. PMID: 23331960 Free PMC article.
-
Predictors of oral anticoagulant-associated adverse events in seniors transitioning from hospital to home: a retrospective cohort study protocol.BMJ Open. 2020 Sep 22;10(9):e036537. doi: 10.1136/bmjopen-2019-036537. BMJ Open. 2020. PMID: 32963065 Free PMC article.
-
Agreement Between Administrative Database and Medical Chart Review for the Prediction of Chronic Kidney Disease G category.Can J Kidney Health Dis. 2020 Oct 10;7:2054358120959908. doi: 10.1177/2054358120959908. eCollection 2020. Can J Kidney Health Dis. 2020. PMID: 33101698 Free PMC article.
-
The increasing burden and complexity of multimorbidity.BMC Public Health. 2015 Apr 23;15:415. doi: 10.1186/s12889-015-1733-2. BMC Public Health. 2015. PMID: 25903064 Free PMC article.
References
-
- Tu Jack V, Austin Peter, Naylor C David, Iron Karey, Zhang Hua. Acute myocardial outcomes in Ontario. In: Naylor C, Slaughter P, editors. Cardiovascular health and services in Ontario: an ICES Atlas. 1999. pp. 83–110. http://www.ices.on.ca/file/7_CVA_Chapter5.pdf.
-
- Jong Philip, Gong Yanyan, Liu Peter P, Austin Peter C, Lee Douglas S, Tu Jack V. Care and outcomes of patients newly hospitalized for heart failure in the community treated by cardiologists compared with other specialists. Circulation. 2003 Jul 15;108(2):184–191. doi: 10.1161/01.CIR.0000080290.39027.48. - DOI - PubMed
-
- Hill M D, Yiannakoulias N, Jeerakathil T, Tu J V, Svenson L W, Schopflocher D P. The high risk of stroke immediately after transient ischemic attack: a population-based study. Neurology. 2004 Jun 8;62(11):2015–2020. - PubMed
LinkOut - more resources
Full Text Sources