

Orthotopic liver transplantation for patients with hepatitis B virus-related liver disease
- PMID: 2010156
- PMCID: PMC2972630
Orthotopic liver transplantation for patients with hepatitis B virus-related liver disease
Abstract
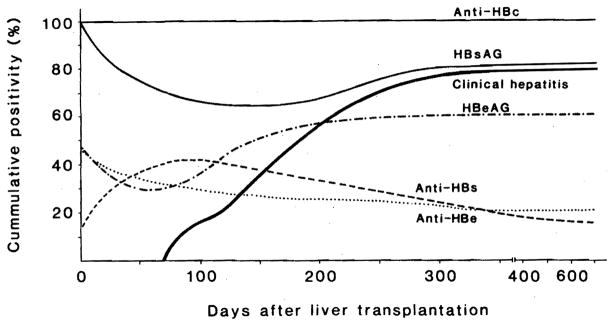
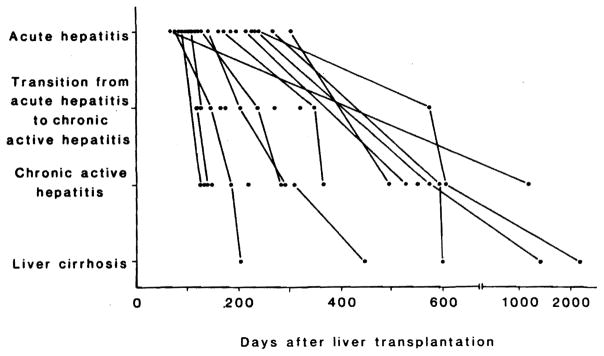
Fifty-nine patients with prior hepatitis B virus infection underwent orthotopic liver transplantation. During the first 2 mo, mortality was not significantly different in the hepatitis B virus-infected group (25.5%) vs. a hepatitis B virus-immune control group (21%). Beyond 2 mo, the mortality, rate of graft loss, need for retransplantation and incidence of abnormal liver function were significantly higher in the hepatitis B virus-infected group. Treatment of the hepatitis B virus infection was attempted with passive immunization, combined active and passive immunization, alpha-interferon or nothing. The clinical outcome was not significantly influenced by any of these therapies. However, of the patients who lived more than 60 days, 6 of 22 treated with active plus passive immunization were cleared of HBsAg, something achieved once in 16 patients treated with alpha-interferon, never in 3 patients with passive immunization only and once in 4 patients with no therapy. In patients with recurrent hepatitis B virus infection, the pace of hepatitis development in the graft appeared to be accelerated, and this was particularly striking in patients who underwent multiple retransplantations at progressively shorter intervals. None of the patients who became HBsAg-negative had HBeAg preoperatively.
Figures


Comment in
-
Liver transplantation for patients with hepatitis B: what have we learned from our results?Hepatology. 1991 Apr;13(4):796-9. Hepatology. 1991. PMID: 2010175 No abstract available.
References
-
- Rizzetto M, Macagno S, Chiaberge E, Verme G, Negro F, Marinucci G, DiGiacomo C, et al. Liver transplantation in hepatitis delta virus disease. Lancet. 1987;2:469–471. - PubMed
-
- Muller R, Lauchart W, Farle M, Klein H, Niehoff G, Pichlmayr R. Simultaneous passive-active immunization for preventing hepatitis B virus reinfection in hepatitis B surface antigen-positive liver transplantation recipients. In: Zuckerman AJ, editor. Viral hepatitis and liver disease. New York: Alan R. Liss, Inc; 1988. pp. 810–812.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical