

Endoscope-guided pneumatic dilation for treatment of esophageal achalasia
- PMID: 20101764
- PMCID: PMC2811791
- DOI: 10.3748/wjg.v16.i4.411
Endoscope-guided pneumatic dilation for treatment of esophageal achalasia
Abstract
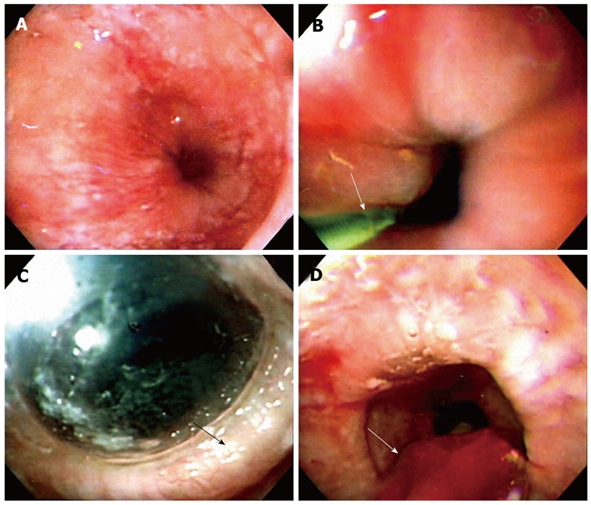
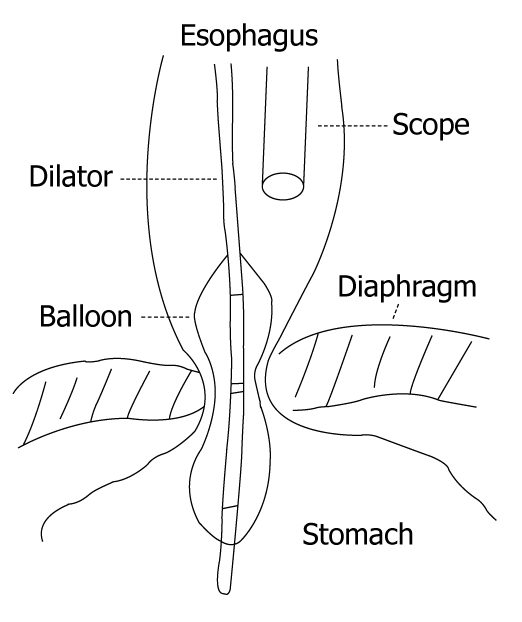
Pneumatic dilation (PD) is considered to be the first line nonsurgical therapy for achalasia. The principle of the procedure is to weaken the lower esophageal sphincter by tearing its muscle fibers by generating radial force. The endoscope-guided procedure is done without fluoroscopic control. Clinicians usually use a low-compliance balloon such as Rigiflex dilator to perform endoscope-guided PD for the treatment of esophageal achalasia. It has the advantage of determining mucosal injury during the dilation process, so that a repeat endoscopy is not needed to assess the mucosal tearing. Previous studies have shown that endoscope-guided PD is an efficient and safe nonsurgical therapy with results that compare well with other treatment modalities. Although the results may be promising, long-term follow-up is required in the near future.
Figures
References
-
- Gockel I, Eckardt VF, Schmitt T, Junginger T. Pseudoachalasia: a case series and analysis of the literature. Scand J Gastroenterol. 2005;40:378–385. - PubMed
-
- Mohamed A. Education and Imaging. Gastrointestinal: pseudoachalasia caused by a lower esophageal stromal tumor. J Gastroenterol Hepatol. 2009;24:1152. - PubMed
-
- Moorman AJ, Oelschlager BK, Rulyak SJ. Pseudoachalasia caused by retroperitoneal B-cell lymphoma. Clin Gastroenterol Hepatol. 2008;6:A32. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
