

Predictors of short-term (seven-day) cardiac outcomes after emergency department visit for syncope
- PMID: 20102895
- PMCID: PMC2821329
- DOI: 10.1016/j.amjcard.2009.08.654
Predictors of short-term (seven-day) cardiac outcomes after emergency department visit for syncope
Abstract
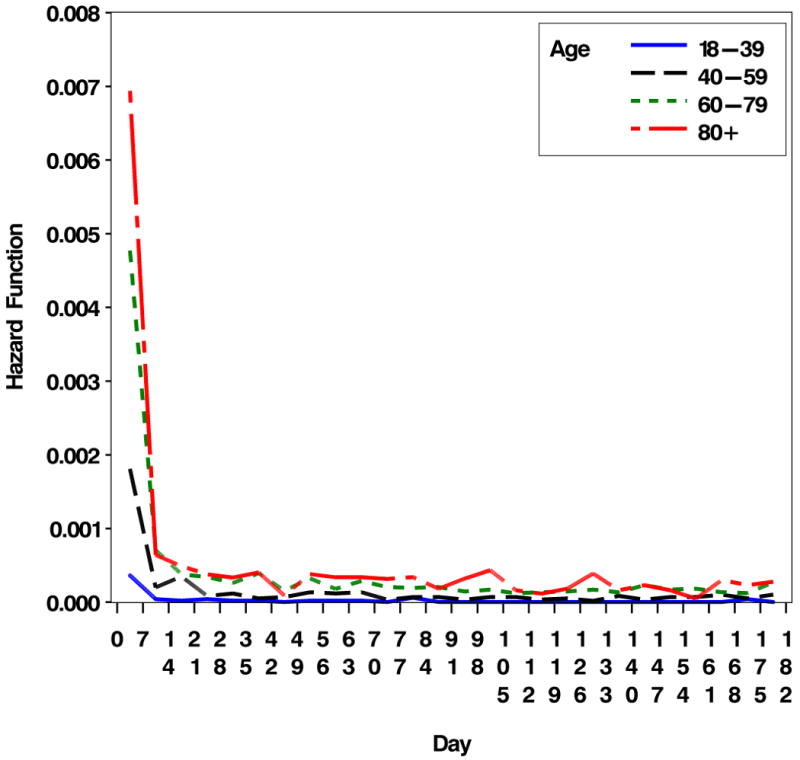
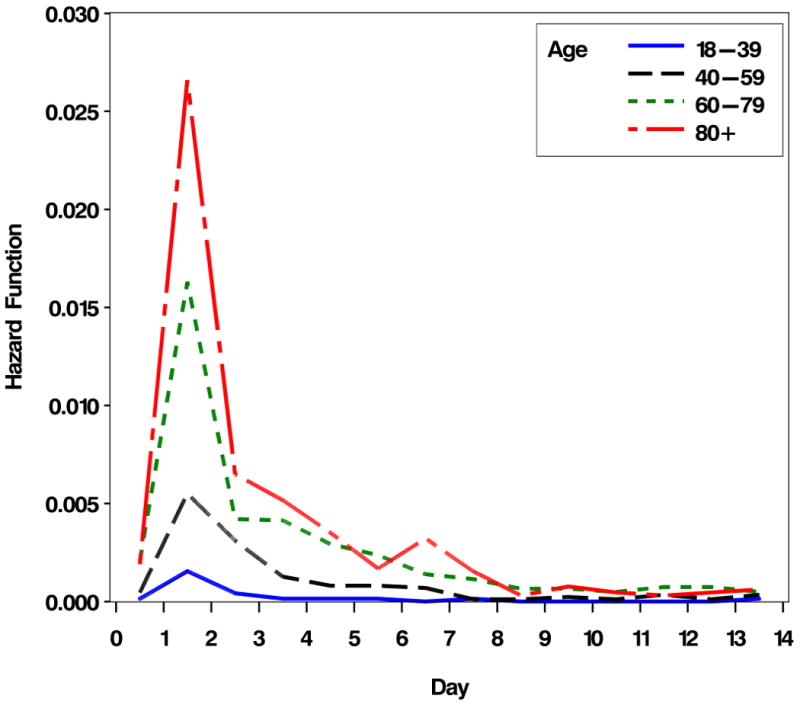
Syncope is a common reason for emergency department (ED) visits, and patients are often admitted to exclude syncope of cardiovascular origin. Population-based data on patterns and predictors of cardiac outcomes may improve decision-making. Our objective was to identify patterns and predictors of short-term cardiac outcomes in ED patients with syncope. Administrative data from an integrated health system of 11 Southern California EDs were used to identify cardiac outcomes after ED presentation for syncope from January 1, 2002, to December 31, 2005. Syncope and cause of death were identified by codes from the International Classification of Disease, Ninth Revision. Cardiac outcomes included cardiac death and hospitalization or procedure consistent with ischemic heart disease, valvular disease, or arrhythmia. Predictors of cardiac outcomes were identified through multivariate logistic regression. There were 35,330 adult subjects who accounted for 39,943 ED visits for syncope. Risk of cardiac outcome sharply decreased following the 7 days after syncope. A 7-day cardiac outcome occurred in 893 cases (3%). Positive predictors of 7-day cardiac outcomes included age > or =60 years, male gender, congestive heart failure, ischemic heart disease, cardiac arrhythmia, and valvular heart disease. Negative predictors included dementia, pacemaker, coronary revascularization, and cerebrovascular disease. There was an age-dependent relation between 7-day cardiac outcomes and arrhythmia and valvular disease, with younger patients (<60 years of age) having greater risk of an event compared to their same-age counterparts. In conclusion, ED decision-making should focus on risk of cardiac event in the first 7 days after syncope and special attention should be given to younger patients with cardiac co-morbidities.
Figures
Similar articles
-
ECG Predictors of Cardiac Arrhythmias in Older Adults With Syncope.Ann Emerg Med. 2018 Apr;71(4):452-461.e3. doi: 10.1016/j.annemergmed.2017.11.014. Epub 2017 Dec 21. Ann Emerg Med. 2018. PMID: 29275946 Free PMC article.
-
Duration of Electrocardiographic Monitoring of Emergency Department Patients With Syncope.Circulation. 2019 Mar 12;139(11):1396-1406. doi: 10.1161/CIRCULATIONAHA.118.036088. Circulation. 2019. PMID: 30661373
-
Patterns and preexisting risk factors of 30-day mortality after a primary discharge diagnosis of syncope or near syncope.Acad Emerg Med. 2012 May;19(5):488-96. doi: 10.1111/j.1553-2712.2012.01336.x. Acad Emerg Med. 2012. PMID: 22594351 Free PMC article.
-
Emergency department factors associated with survival after sudden cardiac arrest.Resuscitation. 2013 Mar;84(3):292-7. doi: 10.1016/j.resuscitation.2012.10.013. Epub 2012 Oct 24. Resuscitation. 2013. PMID: 23103887 Review.
-
Incidence, etiology and predictors of adverse outcomes in 43,315 patients presenting to the Emergency Department with syncope: an international meta-analysis.Int J Cardiol. 2013 Jul 15;167(1):57-62. doi: 10.1016/j.ijcard.2011.11.083. Epub 2011 Dec 20. Int J Cardiol. 2013. PMID: 22192287 Review.
Cited by
-
The Characteristics of Syncope-Related Emergency Department Visits: Resource Utilization and Admission Rate Patterns in Emergency Departments.Cureus. 2022 Feb 8;14(2):e22039. doi: 10.7759/cureus.22039. eCollection 2022 Feb. Cureus. 2022. PMID: 35340474 Free PMC article.
-
Standardized reporting guidelines for emergency department syncope risk-stratification research.Acad Emerg Med. 2012 Jun;19(6):694-702. doi: 10.1111/j.1553-2712.2012.01375.x. Acad Emerg Med. 2012. PMID: 22687184 Free PMC article.
-
Predictors of Short-Term Outcomes after Syncope: A Systematic Review and Meta-Analysis.West J Emerg Med. 2018 May;19(3):517-523. doi: 10.5811/westjem.2018.2.37100. Epub 2018 Mar 13. West J Emerg Med. 2018. PMID: 29760850 Free PMC article.
-
Emergency Department Increased use of Observation Care for Elderly Medicare Patients.J Hosp Adm. 2018 Jun;7(3):9-16. doi: 10.5430/jha.v7n3p9. J Hosp Adm. 2018. PMID: 29736199 Free PMC article.
-
Standardized approaches to syncope evaluation for reducing hospital admissions and costs in overcrowded emergency departments.Yonsei Med J. 2013 Sep;54(5):1110-8. doi: 10.3349/ymj.2013.54.5.1110. Yonsei Med J. 2013. PMID: 23918559 Free PMC article.
References
-
- Colivicchi F, Ammirati F, Melina D, Guido V, Imperoli G, Santini M. Development and prospective validation of a risk stratification system for patients with syncope in the emergency department: the OESIL risk score. Eur Heart J. 2003;24:811–819. - PubMed
-
- Kapoor WN, Karpf M, Wieand S, Peterson JR, Levey GS. A prospective evaluation and follow-up of patients with syncope. N Engl J Med. 1983;309:197–204. - PubMed
-
- Martin TP, Hanusa BH, Kapoor WN. Risk stratification of patients with syncope. Ann Emerg Med. 1997;29:459–466. - PubMed
-
- Sarasin FP, Hanusa BH, Perneger T, Louis-Simonet M, Rajeswaran A, Kapoor WN. A risk score to predict arrhythmias in patients with unexplained syncope. Acad Emerg Med. 2003;10:1312–1317. - PubMed
