

Height adjustment in assessing dual energy x-ray absorptiometry measurements of bone mass and density in children
- PMID: 20103654
- PMCID: PMC2841534
- DOI: 10.1210/jc.2009-2057
Height adjustment in assessing dual energy x-ray absorptiometry measurements of bone mass and density in children
Abstract
Context: In children, bone mineral content (BMC) and bone mineral density (BMD) measurements by dual-energy x-ray absorptiometry (DXA) are affected by height status. No consensus exists on how to adjust BMC or BMD (BMC/BMD) measurements for short or tall stature.
Objective: The aim of this study was to compare various methods to adjust BMC/BMD for height in healthy children.
Design: Data from the Bone Mineral Density in Childhood Study (BMDCS) were used to develop adjustment methods that were validated using an independent cross-sectional sample of healthy children from the Reference Data Project (RDP).
Setting: We conducted the study in five clinical centers in the United States.
Participants: We included 1546 BMDCS and 650 RDP participants (7 to 17 yr of age, 50% female).
Intervention: No interventions were used.
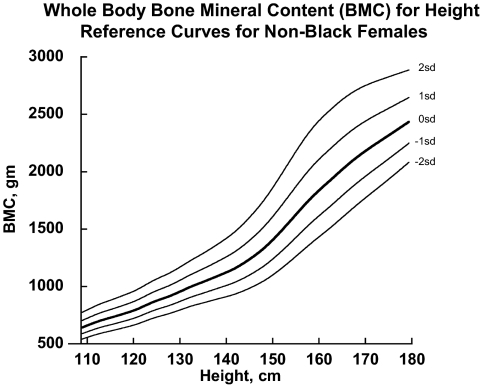
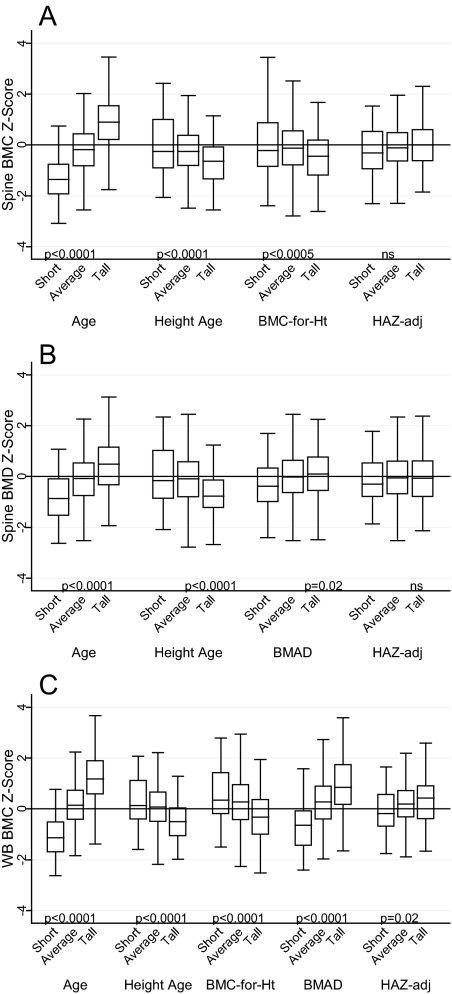
Main outcome measures: We measured spine and whole body (WB) BMC and BMD Z-scores for age (BMC/BMD(age)), height age (BMC/BMD(height age)), height (BMC(height)), bone mineral apparent density (BMAD(age)), and height-for-age Z-score (HAZ) (BMC/BMD(haz)).
Results: Spine and WB BMC/BMD(age)Z and BMAD(age)Z were positively (P < 0.005; r = 0.11 to 0.64) associated with HAZ. Spine BMD(haz) and BMC(haz)Z were not associated with HAZ; WB BMC(haz)Z was modestly associated with HAZ (r = 0.14; P = 0.0003). All other adjustment methods were negatively associated with HAZ (P < 0.005; r = -0.20 to -0.34). The deviation between adjusted and BMC/BMD(age) Z-scores was associated with age for most measures (P < 0.005) except for BMC/BMD(haz).
Conclusions: Most methods to adjust BMC/BMD Z-scores for height were biased by age and/or HAZ. Adjustments using HAZ were least biased relative to HAZ and age and can be used to evaluate the effect of short or tall stature on BMC/BMD Z-scores.
Figures

References
-
- Leonard MB, Zemel BS 2002 Current concepts in pediatric bone disease. Pediatr Clin North Am 49:143–173 - PubMed
-
- Heaney RP 2003 Bone mineral content, not bone mineral density, is the correct bone measure for growth studies. Am J Clin Nutr 78:350–351; author reply 351–352 - PubMed
-
- Leonard MB, Shults J, Elliott DM, Stallings VA, Zemel BS 2004 Interpretation of whole body dual energy x-ray absorptiometry measures in children: comparison with peripheral quantitative computed tomography. Bone 34:1044–1052 - PubMed
-
- Prentice A, Parsons TJ, Cole TJ 1994 Uncritical use of bone mineral density in absorptiometry may lead to size-related artifacts in the identification of bone mineral determinants. Am J Clin Nutr 60:837–842 - PubMed
-
- Gordon CM, Bachrach LK, Carpenter TO, Crabtree N, El-Hajj Fuleihan G, Kutilek S, Lorenc RS, Tosi LL, Ward KA, Ward LM, Kalkwarf HJ 2008 Dual energy x-ray absorptiometry interpretation and reporting in children and adolescents: the 2007 ISCD Pediatric Official Positions. J Clin Densitom 11:43–58 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
