

Do non-targeted effects increase or decrease low dose risk in relation to the linear-non-threshold (LNT) model?
- PMID: 20105434
- PMCID: PMC3076714
- DOI: 10.1016/j.mrfmmm.2010.01.008
Do non-targeted effects increase or decrease low dose risk in relation to the linear-non-threshold (LNT) model?
Abstract
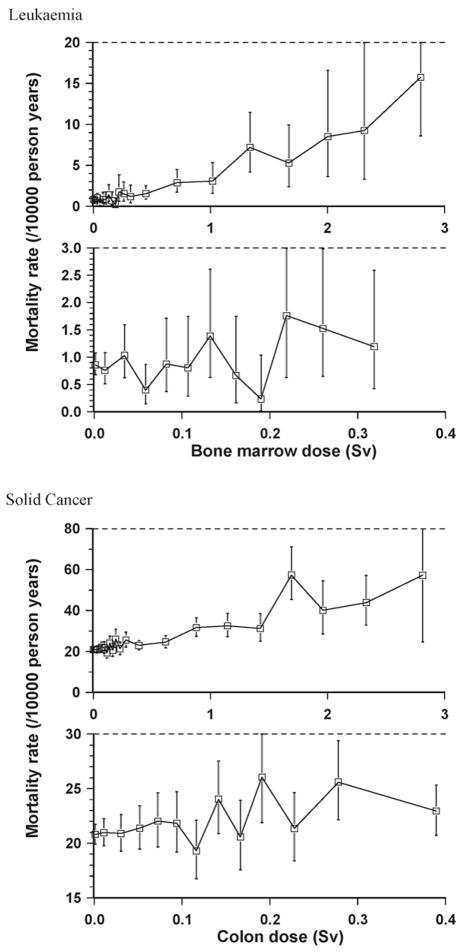
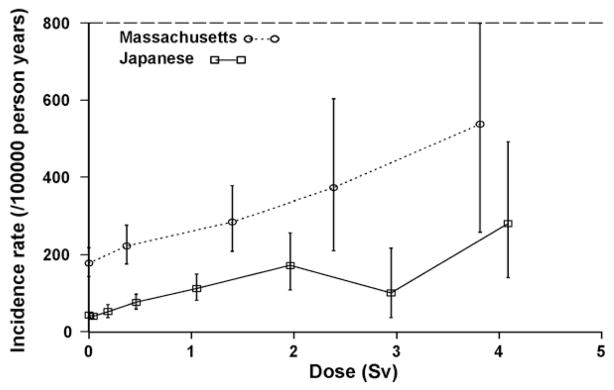
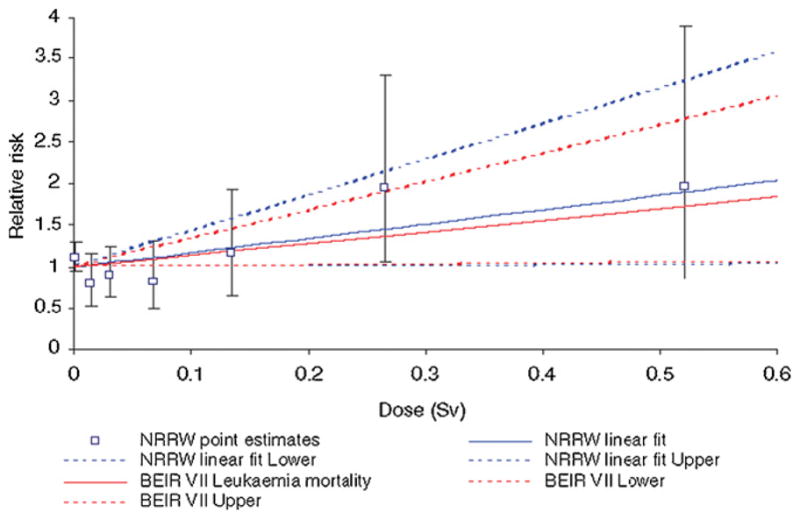
In this paper we review the evidence for departure from linearity for malignant and non-malignant disease and in the light of this assess likely mechanisms, and in particular the potential role for non-targeted effects. Excess cancer risks observed in the Japanese atomic bomb survivors and in many medically and occupationally exposed groups exposed at low or moderate doses are generally statistically compatible. For most cancer sites the dose-response in these groups is compatible with linearity over the range observed. The available data on biological mechanisms do not provide general support for the idea of a low dose threshold or hormesis. This large body of evidence does not suggest, indeed is not statistically compatible with, any very large threshold in dose for cancer, or with possible hormetic effects, and there is little evidence of the sorts of non-linearity in response implied by non-DNA-targeted effects. There are also excess risks of various types of non-malignant disease in the Japanese atomic bomb survivors and in other groups. In particular, elevated risks of cardiovascular disease, respiratory disease and digestive disease are observed in the A-bomb data. In contrast with cancer, there is much less consistency in the patterns of risk between the various exposed groups; for example, radiation-associated respiratory and digestive diseases have not been seen in these other (non-A-bomb) groups. Cardiovascular risks have been seen in many exposed populations, particularly in medically exposed groups, but in contrast with cancer there is much less consistency in risk between studies: risks per unit dose in epidemiological studies vary over at least two orders of magnitude, possibly a result of confounding and effect modification by well known (but unobserved) risk factors. In the absence of a convincing mechanistic explanation of epidemiological evidence that is, at present, less than persuasive, a cause-and-effect interpretation of the reported statistical associations for cardiovascular disease is unreliable but cannot be excluded. Inflammatory processes are the most likely mechanism by which radiation could modify the atherosclerotic disease process. If there is to be modification by low doses of ionizing radiation of cardiovascular disease through this mechanism, a role for non-DNA-targeted effects cannot be excluded.
Copyright 2010 Elsevier B.V. All rights reserved.
Conflict of interest statement
None.
Figures

Similar articles
-
Cancer and non-cancer effects in Japanese atomic bomb survivors.J Radiol Prot. 2009 Jun;29(2A):A43-59. doi: 10.1088/0952-4746/29/2A/S04. Epub 2009 May 19. J Radiol Prot. 2009. PMID: 19454804 Review.
-
Low- and moderate-dose non-cancer effects of ionizing radiation in directly exposed individuals, especially circulatory and ocular diseases: a review of the epidemiology.Int J Radiat Biol. 2021;97(6):782-803. doi: 10.1080/09553002.2021.1876955. Epub 2021 Feb 26. Int J Radiat Biol. 2021. PMID: 33471563 Free PMC article. Review.
-
A review of non-cancer effects, especially circulatory and ocular diseases.Radiat Environ Biophys. 2013 Nov;52(4):435-49. doi: 10.1007/s00411-013-0484-7. Epub 2013 Aug 1. Radiat Environ Biophys. 2013. PMID: 23903347 Free PMC article. Review.
-
Non-cancer diseases and non-targeted effects.Mutat Res. 2010 May 1;687(1-2):73-77. doi: 10.1016/j.mrfmmm.2010.01.007. Epub 2010 Jan 25. Mutat Res. 2010. PMID: 20097211
-
Are cancer risks associated with exposures to ionising radiation from internal emitters greater than those in the Japanese A-bomb survivors?Radiat Environ Biophys. 2007 Nov;46(4):299-310. doi: 10.1007/s00411-007-0122-3. Epub 2007 Jul 17. Radiat Environ Biophys. 2007. PMID: 17639450
Cited by
-
Alternative medicine techniques have non-linear effects on radiation response and can alter the expression of radiation induced bystander effects.Dose Response. 2013;11(1):82-98. doi: 10.2203/dose-response.11-048.Mothersill. Epub 2012 Jan 20. Dose Response. 2013. PMID: 23550268 Free PMC article.
-
Sources of contradictions in the evaluation of population genetic consequences after the chernobyl disaster.Acta Naturae. 2013 Jan;5(1):47-62. Acta Naturae. 2013. PMID: 23556130 Free PMC article.
-
The Radiation Exposure of Radiographer Related to the Location in C-arm Fluoroscopy-guided Pain Interventions.Korean J Pain. 2014 Apr;27(2):162-7. doi: 10.3344/kjp.2014.27.2.162. Epub 2014 Mar 28. Korean J Pain. 2014. PMID: 24748945 Free PMC article.
-
Long-term effects of ionising radiation on the brain: cause for concern?Radiat Environ Biophys. 2013 Mar;52(1):5-16. doi: 10.1007/s00411-012-0436-7. Epub 2012 Oct 26. Radiat Environ Biophys. 2013. PMID: 23100112 Review.
-
Uncomfortable issues in radiation protection posed by low-dose radiobiology.Radiat Environ Biophys. 2013 Aug;52(3):293-8. doi: 10.1007/s00411-013-0472-y. Epub 2013 May 15. Radiat Environ Biophys. 2013. PMID: 23673925
References
-
- Stevens LG. Injurious effects on the skin. Br Med J. 1896;1:998.
-
- Gilchrist TC. A case of dermatitis due to the X-rays. Bull Johns Hopkins Hosp. 1897;8(71):17–22.
-
- Frieben A. Demonstration eines Cancroids des rechten Handrückens, das sich nach langdauernder Einwirkung von Röntgenstrahlen bei einem 33 jährigen Mann entwickelt hatte. Fortschr Röntgenstr. 1902;6:106.
-
- U.S. National Academy of Sciences. Health Risks from Exposure to Low Levels of Ionizing Radiation. BEIR VII Phase 2. The National Academies Press; Washington, DC: 2006. National Research Council Committee to assess health risks from exposure to low levels of ionizing radiation.
-
- International Commission on Radiological Protection, ICRP Publication 103 ICRP Publication 103. Annals ICRP. 2–4. Vol. 37. Pergamon; Oxford: 2007. The 2007 recommendations of the International Commission on Radiological Protection; pp. 1–332. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
