

Outcomes in children with intestinal failure following listing for intestinal transplant
- PMID: 20105588
- PMCID: PMC2813842
- DOI: 10.1016/j.jpedsurg.2009.10.019
Outcomes in children with intestinal failure following listing for intestinal transplant
Abstract
Purpose: The purpose of this study was to describe the population of pediatric patients waiting for intestinal transplant and to evaluate the risk of death or transplant by specific disease states.
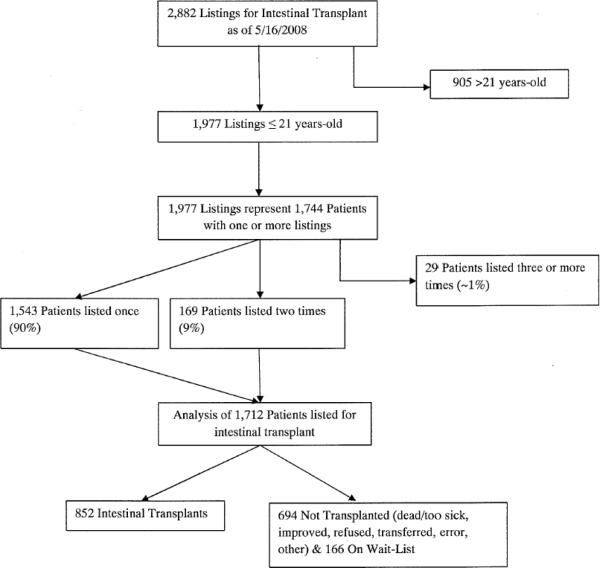
Methods: We studied the United Network for Organ Sharing (UNOS) database (Jan 1,1991 to 5/16/08) for patients 21 years old or younger at first listing for intestinal transplant and examined their age, sex, weight, and diagnoses. Time to list removal was summarized with cumulative incidence curves. Multinomial logistic regression was used to compare relative risk ratios for removal from the list for transplant, death, or other reasons.
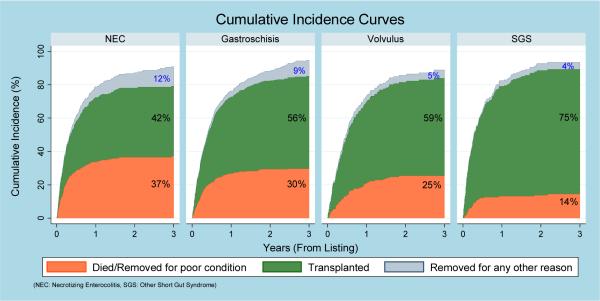
Results: We identified 1712 children listed for intestinal transplant (57% male, 51% <1 year, weight 8.1 kg [IQR, 6.1-14.1] at listing). Median age and weight at transplant (n = 852) were 1 year (IQR, 1-5) and 10 kg (IQR, 6.5-16.3). Regression analysis demonstrated significant differences in outcomes among disease conditions (P < .001). Compared to the gastroschisis group, the relative risk ratio for death versus transplant was higher in the necrotizing enterocolitis group (P = .015), lower in the short gut syndrome group (P = .001), and not different in the volvulus group (P = .94) after adjustment for weight and sex.
Conclusions: We conclude that the relative risk of transplant vs death varies significantly by the disease condition of the patient.
Copyright 2010 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
The role of intestinal transplantation in the management of babies with extensive gut resections.J Pediatr Surg. 2003 Feb;38(2):145-9. doi: 10.1053/jpsu.2003.50033. J Pediatr Surg. 2003. PMID: 12596093
-
Long-term outcomes of short bowel syndrome requiring long-term/home intravenous nutrition compared in children with gastroschisis and those with volvulus.Transplant Proc. 2010 Jan-Feb;42(1):5-8. doi: 10.1016/j.transproceed.2009.12.033. Transplant Proc. 2010. PMID: 20172269
-
Intestinal transplantation for short bowel syndrome secondary to gastroschisis.J Pediatr Surg. 2006 Nov;41(11):1841-5. doi: 10.1016/j.jpedsurg.2006.06.010. J Pediatr Surg. 2006. PMID: 17101355
-
The UNOS OPTN waiting list: 1988 to 1994. United Network for Organ Sharing. Organ Procurement and Transplantation Network.Clin Transpl. 1994:69-86. Clin Transpl. 1994. PMID: 7547588 Review.
-
Preserving bowel length with a transluminal stent in neonates with multiple intestinal anastomoses: a case series and review of the literature.J Pediatr Surg. 2011 Jul;46(7):1368-72. doi: 10.1016/j.jpedsurg.2011.01.011. J Pediatr Surg. 2011. PMID: 21763836 Review.
Cited by
-
Experimental Assessment of Intestinal Damage in Controlled Donation After Circulatory Death for Visceral Transplantation.Transpl Int. 2023 Jan 12;36:10803. doi: 10.3389/ti.2023.10803. eCollection 2023. Transpl Int. 2023. PMID: 36713114 Free PMC article.
-
Preclinical Study of DCD and Normothermic Perfusion for Visceral Transplantation.Transpl Int. 2023 Sep 8;36:11518. doi: 10.3389/ti.2023.11518. eCollection 2023. Transpl Int. 2023. PMID: 37745640 Free PMC article.
-
Multidrug-resistant organisms: A significant cause of severe sepsis in pediatric intestinal and multi-visceral transplantation.Am J Transplant. 2022 Jan;22(1):122-129. doi: 10.1111/ajt.16756. Epub 2021 Jul 28. Am J Transplant. 2022. PMID: 34245113 Free PMC article.
-
Overview of Physical, Neurocognitive, and Psychosocial Outcomes in Pediatric Intestinal Failure and Transplantation.Curr Gastroenterol Rep. 2022 Nov;24(11):145-155. doi: 10.1007/s11894-022-00848-3. Epub 2022 Aug 30. Curr Gastroenterol Rep. 2022. PMID: 36040624 Review.
-
Clinical outcomes in pediatric intestinal failure: a meta-analysis and meta-regression.Am J Clin Nutr. 2019 Aug 1;110(2):430-436. doi: 10.1093/ajcn/nqz110. Am J Clin Nutr. 2019. PMID: 31172170 Free PMC article.
References
-
- Grant D. Intestinal transplantation: 1997 report of the international registry. Intestinal Transplant Registry. Transplantation. 1999;67(7):1061–4. - PubMed
-
- Harmon WE, McDonald RA, Reyes JD, et al. Pediatric transplantation, 1994–2003. Am J Transplant. 2005;5(4 Pt 2):887–903. - PubMed
-
- Fryer JP. Intestinal transplantation: an update. Curr Opin Gastroenterol. 2005;21(2):162–8. - PubMed
-
- Kaufman SS. Small bowel transplantation: selection criteria, operative techniques, advances in specific immunosuppression, prognosis. Curr Opin Pediatr. 2001;13(5):425–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
