

Genetics of craniosynostosis: review of the literature
- PMID: 20108486
- PMCID: PMC5051481
Genetics of craniosynostosis: review of the literature
Abstract
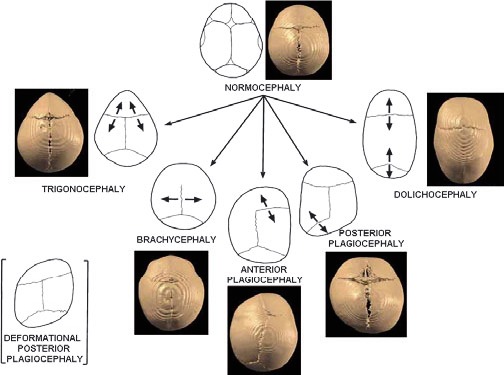
Craniosynostosis represents a defection of the skull caused by early fusion of one or more cranial sutures. The shape alteration of the cranial vault varies, depending on the fused sutures, so that compensatory growth occurs in dimensions not restricted by sutures. Craniosynostosis can be divided into two main groups: syndromic and nonsyndromic. Nonsyndromic craniosynostosis is typically an isolated finding that is classified according to the suture(s) involved. Syndromic craniosynostosis is associated with various dysmorphisms involving the face, skeleton, nervous system and is usually accompanied by developmental delay. In the last 15 years, research on craniosynostosis has progressed from the description of gross abnormalities to the understanding of the genetic basis of certain cranial deformities. Mutations in the genes encoding fibroblast growth factor receptors 1, 2 and 3 (FGFR-1, FGFR-2, FGFR-3), TWIST and MSX2 (muscle segment homebox 2) have been identified in certain syndromic craniosynostosis. The molecular basis of many types of syndromic craniosynostosis is known and diagnostic testing strategies will often lead to a specific diagnosis. Although the clarification of a genetic lesion does not have a direct impact on the management of the patient in many cases, there is a significant benefit in providing accurate prenatal diagnosis. This review summarizes the available knowledge on cranisynostosis and presents a graduated strategy for the genetic diagnosis of these craniofacial defects.
Figures

References
-
- Kathy Chun, Ahmad S. Teebi, Cyrus Azimi, Leslie Steele, Peter N. Ray. Screening of Patients with Craniosynostosis: Molecular Strategy. American Journal of Medical Genetics. 2003;120A:470–473. - PubMed
-
- Cunningham ML, Seto ML, Ratisoontorn C, Heike CL, Hing AV. Syndromic craniosynostosis: from history to hydrogen bonds. Orthod Craniofacial Res. 2007;10:67–81. - PubMed
-
- Vesalius A. De Humani Corporis Fabrica. Nation Library of Medicine. :1543. http://www.nlm.nih.gov/ihm/images/A/26/919.jpg.
-
- Andrew O, M Wilkie. Craniosynostosis: genes and mechanisms. Human Molecular Genetics. 1997;6(10 Review) - PubMed
-
- Kimonis Virginia, Gold JA, Hoffman T, Panchal J, Boyadjiev S. Genetics of Craniosynostosis. Semin Pediatr Neurol. 2007;14:150–161. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous