

The electrocardiographic profile of patients with angina pectoris
- PMID: 20108496
- PMCID: PMC5051487
The electrocardiographic profile of patients with angina pectoris
Abstract
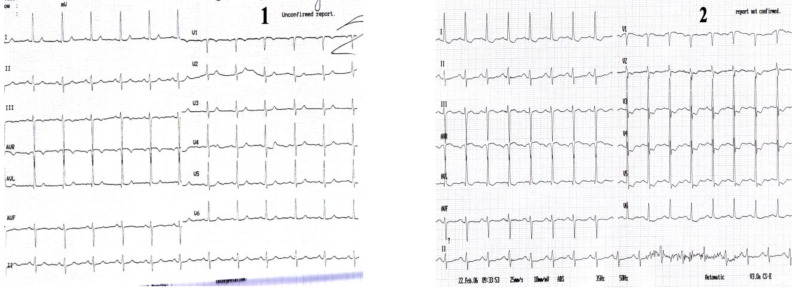
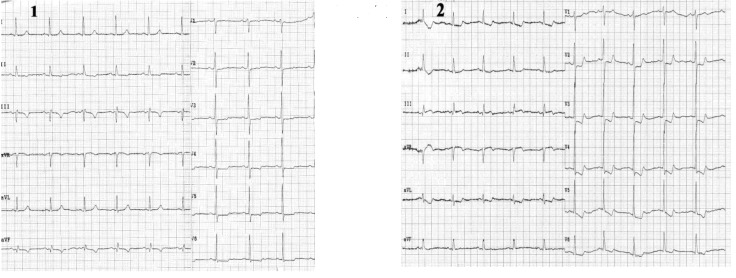
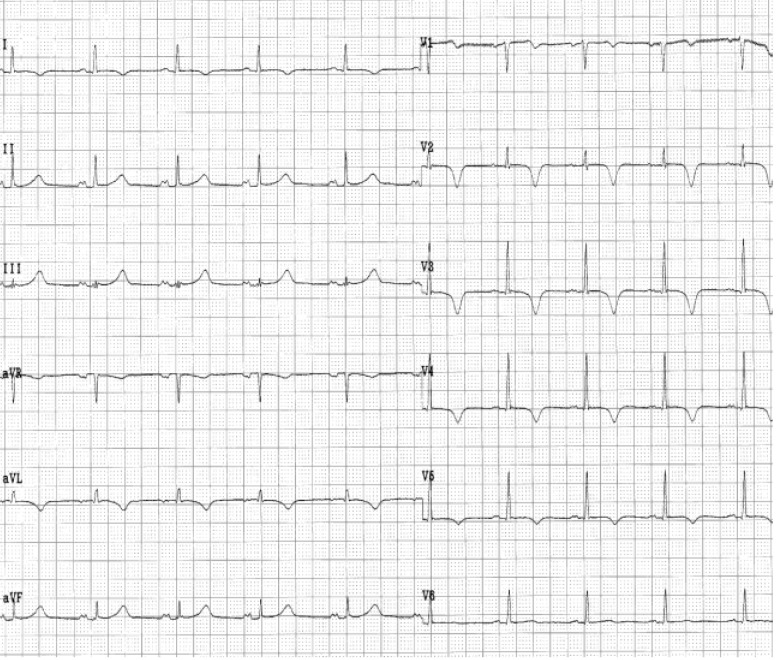
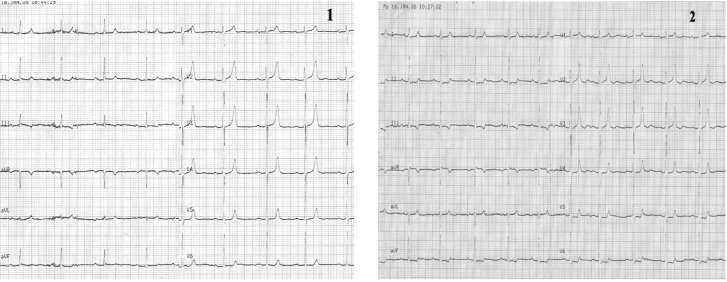
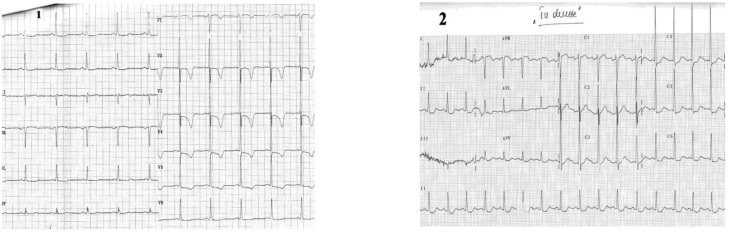
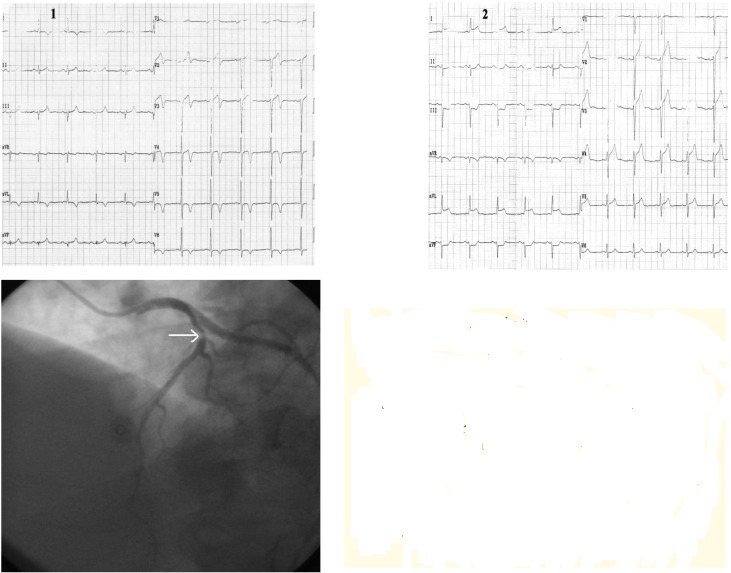
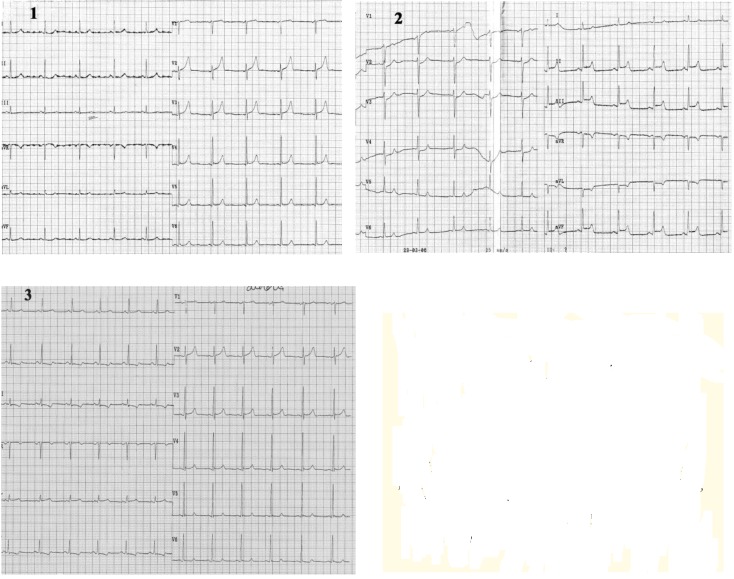
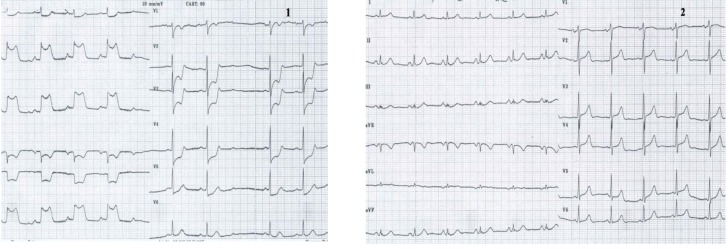
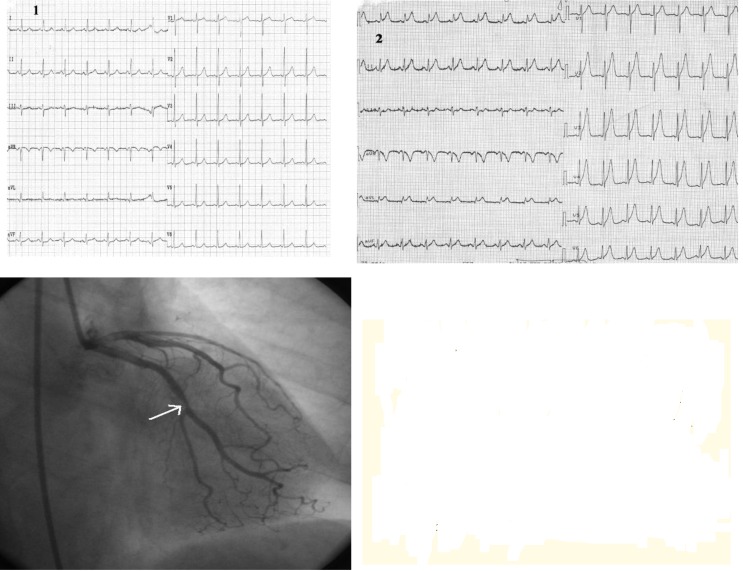
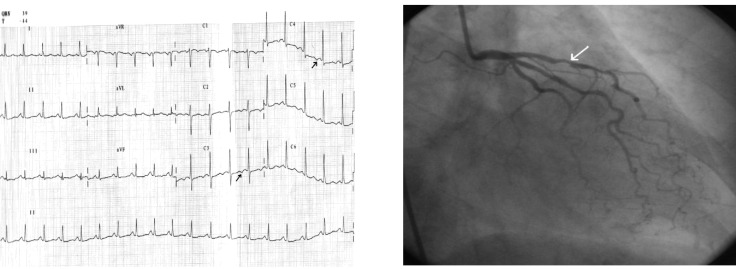
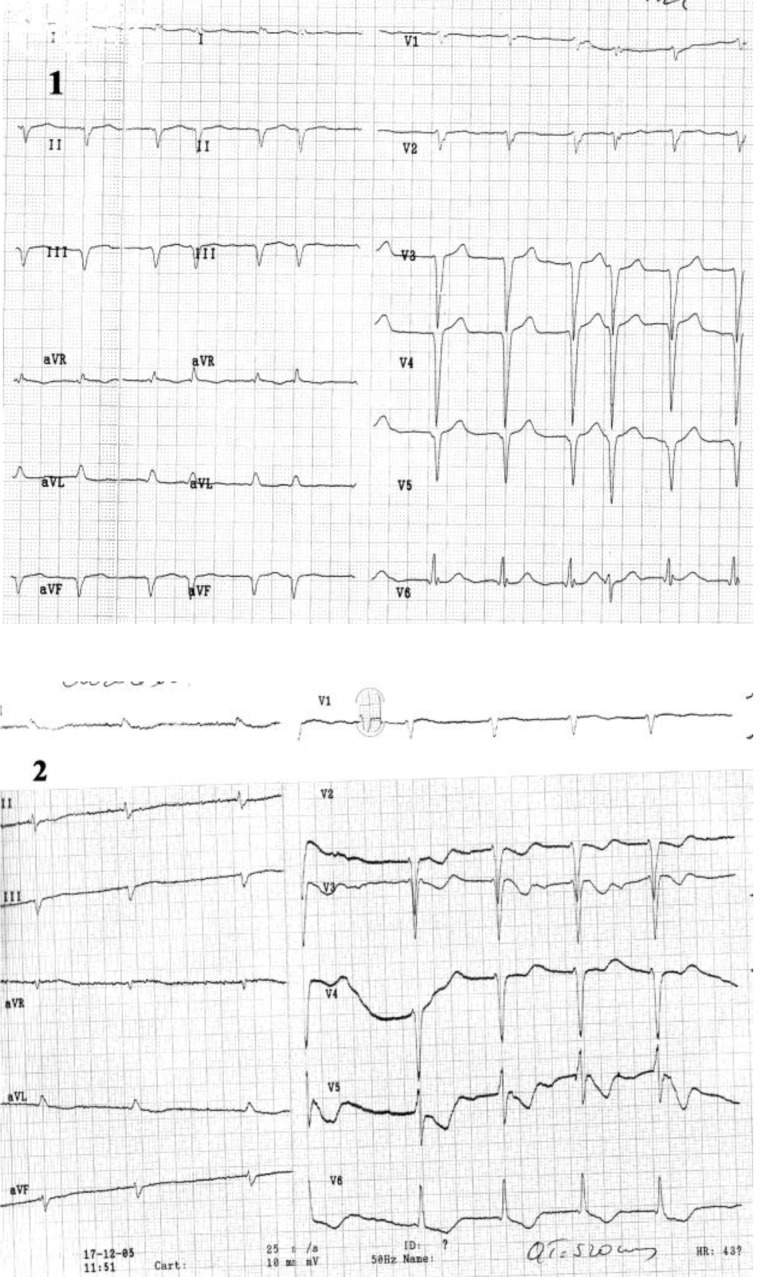
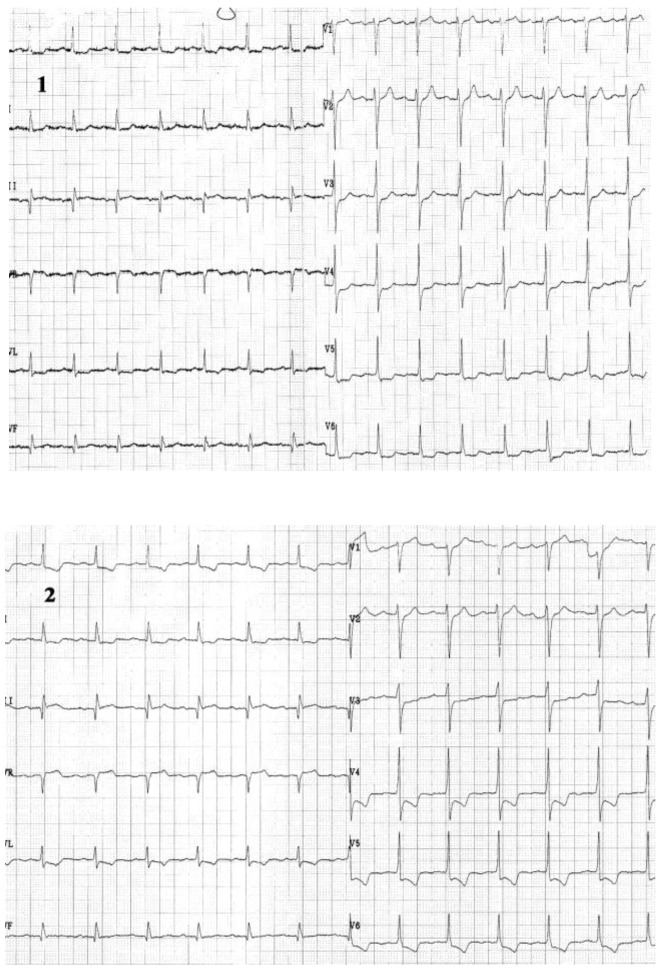
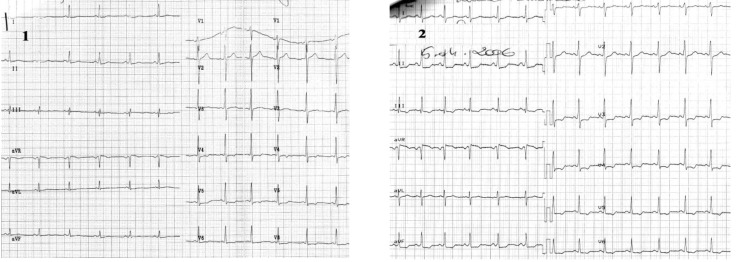
Angina pectoris is a common disabling disorder and a clinical syndrome, caused by myocardial ischemia; an imbalance between myocardial oxygen supply and myocardial oxygen consumption. Thus, ischemia produces a typical series of events such as metabolic and biochemical alterations which lead to impaired ventricular relaxation and diastolic dysfunction, impaired systolic function, and electrocardiographic abnormalities and painful symptoms of angina. Transmembrane ionic currents are responsible for the cardiac potentials that are recorded as the electrocardiogram (ECG). The electrocardiographic profile of patients with angina pectoris is variate. The electrocardiogram provides critical information for both diagnosis and prognosis, particularly when a tracing is obtained during the episodes of pain. A completely normal electrocardiogram does not exclude the possibility of acute coronary syndrome. Serial ECG tracings improve the clinician's ability to diagnose acute and chronic coronary syndromes. The ECG may assist in clarifying the differential diagnosis if taken in the presence of pain. The resting ECG also has an important role in risk stratification. Exercise ECG is more sensitive and specific than the resting ECG as far as myocardial ischemia detection is concerned, and it represents the test of choice which helps identifying inducible ischemia in the majority of patients suspected of stable angina.
Figures

References
-
- C Ginghina, M Marinescu, D Dragomir. Indreptar de diagnostic si tratament in infarctul miocardic acut. 2002:77–123.
-
- Zipes , Libby , Bonow , Braunwald Coronary blood flow and myocardial iaschemia. 2005;44:1103–1107.
-
- Gibbons RJ, Abrams J, Chatterjee K, et al. ACC/AHA 2002 guideline update for the management of patients with chronic stable angina : a report of the American College of Cardiology /American Heart Association Task Force on Practice Guidelines ( Committee to Update the 1999 Guidelines for the Management of Patient with Chronic Stable Angina ) J Am Coll Cardiol. 2003 Jan 1;41(1):159–168. - PubMed
-
- Kim Fox, et al. Guidelines on the management of stable angina pectoris : the task force on the management of stable angina pectoris of the European Society of Cardiology. Eur Heart J. 2006;10:10–93. - PubMed
-
- Diderholm E, Andren B, et al. ST depression in ECG at entry indicates severe coronary lesions and large benefits of an early invasive treatment strategy in unstable coronary artery disease; the FRISC II ECG substudy. The Fast Revascularisation during InStability in Coronary artery disease. Eur Heart J. 2002 Jan;23(1):41–49. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical