

Case Reports
Therapeutical solutions for non-malignant eso-bronchial fistulas
Affiliations
- PMID: 20108499
- PMCID: PMC5051476
Item in Clipboard
Case Reports
Therapeutical solutions for non-malignant eso-bronchial fistulas
J Med Life.
2009 Jan-Mar.
Abstract
We assessed the efficacy of surgical treatment for the patients with eso-respiratory fistulas. The following cases revealed the anesthesic and surgical difficulties, and also intraoperative and postoperative complications that can occur when the esophageal contents get into the respiratory system. In these situations, therapy must be adapted according to fistula's topography and etiology, and also to patients' biological conditions.
Figures

Preoperative X-ray exam - lung opacity at upper right lobe

Preoperative thoracic CT scan upper right lobe suppuration

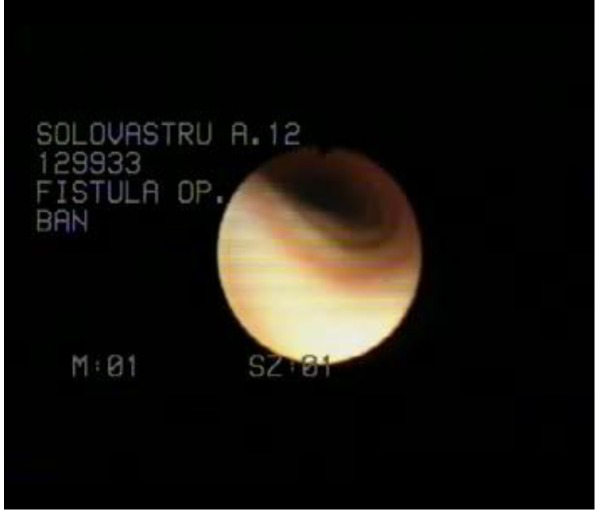
Bronchoscopy – bronchial fistula

Intraoperative aspects: A – upper right lobbectomy;
B – dissection of esophagus and exposure of fistula;
C – esophageal myotomy

Postoperative chest X-ray – complete reexpansion of the right lung

Preoperative esophagography – round esophageal opacity
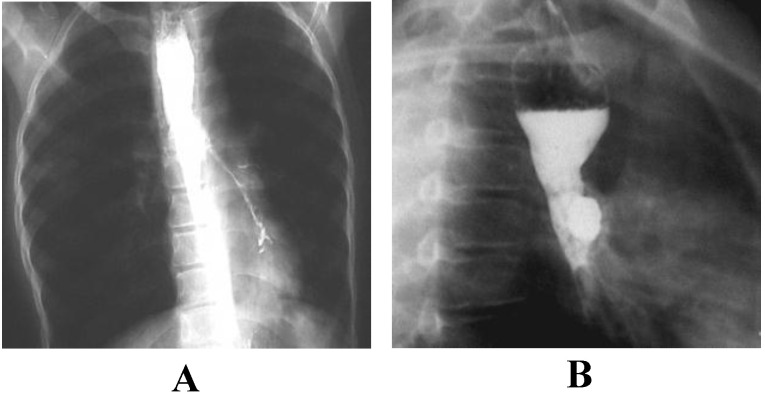
Esophageal barium passage:
A - left eso-bronchial fistula;
B - partial esophageal stenosis with dilatation

Thoracic CT scan: A - left lower lobe pneumonia; B – left eso-bronchial fistula
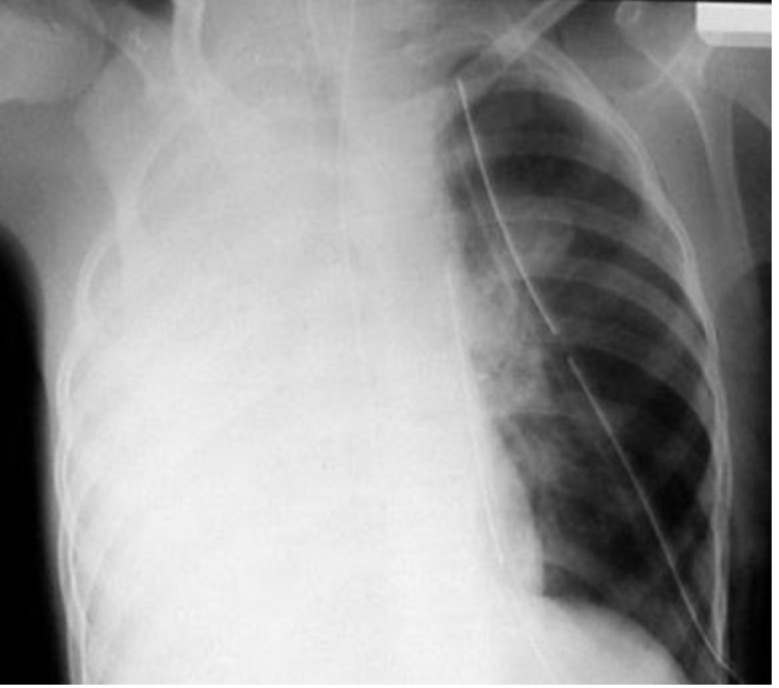
Postoperative chest X-ray: right lung ARDS
Postoperative bronchoscopy at 2 months after
surgery – intermittent stenosis of left main bronchus

Esophageal barium passage – normal

Chest X ray
after re-thoracotomy

Postoperative
thoracic scans

Bronchoscopy after re-thoracotomy - normal aspects

Preoperative CT scan – revealed the eso-tracheal fistula

Intraoperative aspects: A - dissection of esophagus and trachea, revealing the fistula;
B - muscle interposition between esophagus and trachea after resection of fistula
Similar articles
-
[Acquired, benign, nontraumatic esophago-bronchial fistulas].Helv Chir Acta. 1968 Jan;35(1):11-20. Helv Chir Acta. 1968. PMID: 5662299 French. No abstract available.
-
Congenital bronchoesophageal fistula in the adult.Ann Otol Rhinol Laryngol. 1987 Jan-Feb;96(1 Pt 1):65-7. doi: 10.1177/000348948709600116. Ann Otol Rhinol Laryngol. 1987. PMID: 3813387
-
Adult congenital bronchoesophageal fistula.Thorac Cardiovasc Surg. 2007 Aug;55(5):334-6. doi: 10.1055/s-2006-924482. Thorac Cardiovasc Surg. 2007. PMID: 17629871
-
[Bronchoesophageal fistulae: apropos a case rarely seen].Chir Ital. 1992 Jun-Aug;44(3-4):107-14. Chir Ital. 1992. PMID: 1306137 Review. Italian.
-
Outcomes of thoracic endovascular aortic repair for aortobronchial and aortoesophageal fistulas.J Endovasc Ther. 2009 Aug;16(4):428-40. doi: 10.1583/09-2741R.1. J Endovasc Ther. 2009. PMID: 19702348 Review.
References
-
- Monica Kohll, Nikhll Kothari, M.P. Khan. Retrospective study of prognostic factors in esophageal atresia and tracheoesophageal fistula. J Anaesth Clin Pharmacol. 2008;24(4):451–454.
-
- Engum SA, Grosfeld JL, West KW, Rescorla FJ, Scherer LR. 3d Analysis of morbidity and mortality in 227 cases of esophageal atresia and/or tracheoesophageal fistula over two decades. Arch Surg. 1995;130:502–583. - PubMed
-
- Williams J. Diagnosing tracheoesophageal fistula without esophageal atresia. Clin Pediatr (Phila) 1996 Feb;35(2):103–104. - PubMed
-
- Marzelle J, Dartevelle P, Khalife J. Surgical management of acquired post-intubation tracheo-oesophageal fistulas: 27 patients. Eur J Cardiothorac Surg. 1989;3(6):499–502. discussion 502-3. - PubMed
-
- Reed D Mathisen. Tracheoesophageal fistula. Chest Surgery Clinics of North America. 13(2):271–289. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources