

Using genetic algorithms to optimise current and future health planning--the example of ambulance locations
- PMID: 20109172
- PMCID: PMC2828441
- DOI: 10.1186/1476-072X-9-4
Using genetic algorithms to optimise current and future health planning--the example of ambulance locations
Abstract
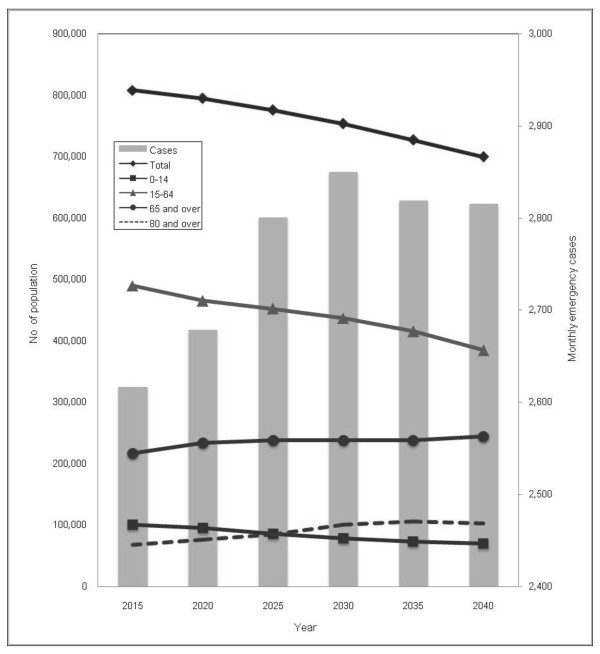
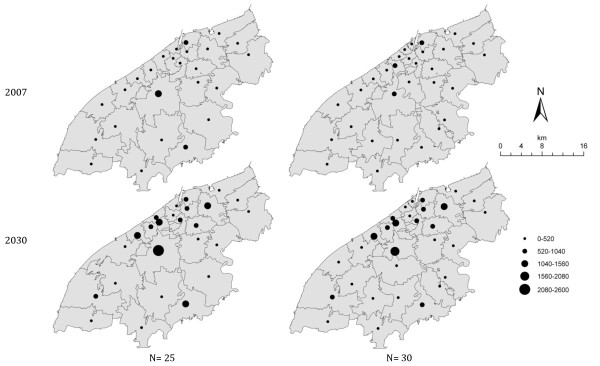
Background: Ambulance response time is a crucial factor in patient survival. The number of emergency cases (EMS cases) requiring an ambulance is increasing due to changes in population demographics. This is decreasing ambulance response times to the emergency scene. This paper predicts EMS cases for 5-year intervals from 2020, to 2050 by correlating current EMS cases with demographic factors at the level of the census area and predicted population changes. It then applies a modified grouping genetic algorithm to compare current and future optimal locations and numbers of ambulances. Sets of potential locations were evaluated in terms of the (current and predicted) EMS case distances to those locations.
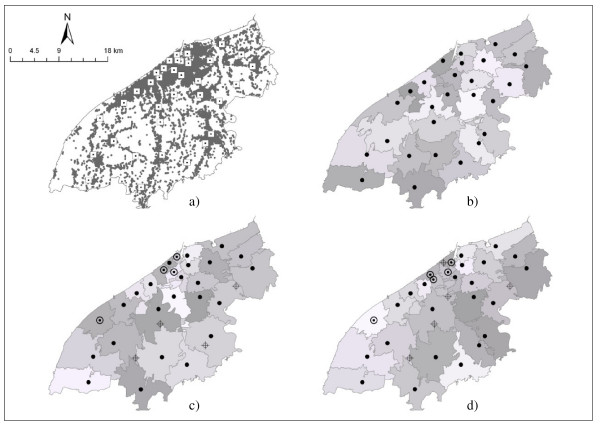
Results: Future EMS demands were predicted to increase by 2030 using the model (R2 = 0.71). The optimal locations of ambulances based on future EMS cases were compared with current locations and with optimal locations modelled on current EMS case data. Optimising the location of ambulance stations locations reduced the average response times by 57 seconds. Current and predicted future EMS demand at modelled locations were calculated and compared.
Conclusions: The reallocation of ambulances to optimal locations improved response times and could contribute to higher survival rates from life-threatening medical events. Modelling EMS case 'demand' over census areas allows the data to be correlated to population characteristics and optimal 'supply' locations to be identified. Comparing current and future optimal scenarios allows more nuanced planning decisions to be made. This is a generic methodology that could be used to provide evidence in support of public health planning and decision making.
Figures
Similar articles
-
EMS relocation in a rural area using a geographic information system can improve response time to motor vehicle crashes.J Trauma. 2011 Oct;71(4):1023-6. doi: 10.1097/TA.0b013e318230f6f0. J Trauma. 2011. PMID: 21986742
-
Optimizing the location of ambulances in Tijuana, Mexico.Comput Biol Med. 2017 Jan 1;80:107-115. doi: 10.1016/j.compbiomed.2016.11.016. Epub 2016 Nov 30. Comput Biol Med. 2017. PMID: 27930929
-
Factors affecting ambulance utilization for asthma attack treatment: understanding where to target interventions.Public Health. 2015 May;129(5):501-8. doi: 10.1016/j.puhe.2015.02.009. Epub 2015 Mar 7. Public Health. 2015. PMID: 25753282
-
Dynamic ambulance relocation: a scoping review.BMJ Open. 2023 Dec 14;13(12):e073394. doi: 10.1136/bmjopen-2023-073394. BMJ Open. 2023. PMID: 38101827 Free PMC article.
-
Ambulance diversion and emergency department offload delay: resource document for the National Association of EMS Physicians position statement.Prehosp Emerg Care. 2011 Oct-Dec;15(4):555-61. doi: 10.3109/10903127.2011.608871. Prehosp Emerg Care. 2011. PMID: 21870947 Review.
Cited by
-
A two-stage spatial allocation model for elderly healthcare facilities in large-scale affordable housing communities: a case study in Nanjing City.Int J Equity Health. 2018 Dec 12;17(1):183. doi: 10.1186/s12939-018-0898-6. Int J Equity Health. 2018. PMID: 30541553 Free PMC article.
-
Optimal Planning of Health Services through Genetic Algorithm and Discrete Event Simulation: A Proposed Model and Its Application to Stroke Rehabilitation Care.MDM Policy Pract. 2022 Oct 22;7(2):23814683221134098. doi: 10.1177/23814683221134098. eCollection 2022 Jul-Dec. MDM Policy Pract. 2022. PMID: 36310567 Free PMC article.
-
A spatial analysis of variations in health access: linking geography, socio-economic status and access perceptions.Int J Health Geogr. 2011 Jul 25;10:44. doi: 10.1186/1476-072X-10-44. Int J Health Geogr. 2011. PMID: 21787394 Free PMC article.
-
A Review and Framework for Categorizing Current Research and Development in Health Related Geographical Information Systems (GIS) Studies.Yearb Med Inform. 2014 Aug 15;9(1):110-24. doi: 10.15265/IY-2014-0008. Yearb Med Inform. 2014. PMID: 25123730 Free PMC article. Review.
-
Delivery of public health interventions by the ambulance sector: a scoping review.BMC Public Health. 2023 Oct 24;23(1):2082. doi: 10.1186/s12889-023-16473-2. BMC Public Health. 2023. PMID: 37875881 Free PMC article.
References
-
- Stiell IG, Wells GA, DeMaio VJ, Spaite DW, Field BJ, Munkley DP, Lyver MB, Luinstra LG, Ward R. Modifiable factors associated with improved cardiac arrest survival in a multicenter BLS-D system: OPALS study phase I results. Ann Emerg Med. 1999;33:44–50. doi: 10.1016/S0196-0644(99)70415-4. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
