

Non-invasive cardiac stress testing before elective major non-cardiac surgery: population based cohort study
- PMID: 20110306
- PMCID: PMC2813428
- DOI: 10.1136/bmj.b5526
Non-invasive cardiac stress testing before elective major non-cardiac surgery: population based cohort study
Abstract
Objective: To determine the association of non-invasive cardiac stress testing before elective intermediate to high risk non-cardiac surgery with survival and hospital stay.
Design: Population based retrospective cohort study.
Setting: Acute care hospitals in Ontario, Canada, between 1 April 1994 and 31 March 2004.
Participants: Patients aged 40 years or older who underwent specific elective intermediate to high risk non-cardiac surgical procedures.
Interventions: Non-invasive cardiac stress testing performed within six months before surgery.
Main outcome measures: Postoperative one year survival and length of stay in hospital.
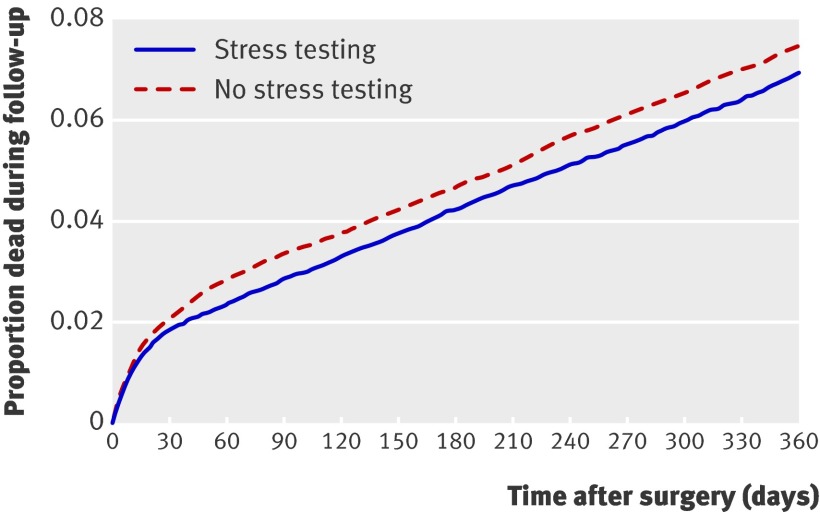
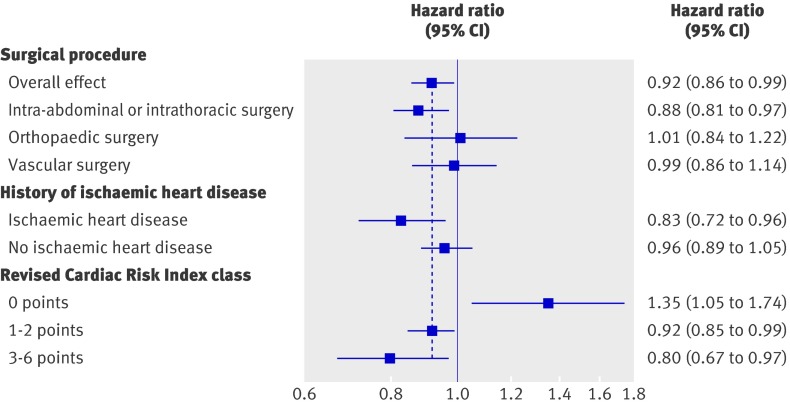
Results: Of the 271 082 patients in the entire cohort, 23 991 (8.9%) underwent stress testing. After propensity score methods were used to reduce important differences between patients who did or did not undergo preoperative stress testing and assemble a matched cohort (n=46 120), testing was associated with improved one year survival (hazard ratio (HR) 0.92, 95% CI 0.86 to 0.99; P=0.03) and reduced mean hospital stay (difference -0.24 days, 95% CI -0.07 to -0.43; P<0.001). In an analysis of subgroups defined by Revised Cardiac Risk Index (RCRI) class, testing was associated with harm in low risk patients (RCRI 0 points: HR 1.35, 95% CI 1.05 to 1.74), but with benefit in patients who were at intermediate risk (RCRI 1-2 points: 0.92, 95% CI 0.85 to 0.99) or high risk (RCRI 3-6 points: 0.80, 95% CI 0.67 to 0.97).
Conclusions: Preoperative non-invasive cardiac stress testing is associated with improved one year survival and length of hospital stay in patients undergoing elective intermediate to high risk non-cardiac surgery. These benefits principally apply to patients with risk factors for perioperative cardiac complications.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Preoperative non-invasive stress testing.BMJ. 2010 Jan 18;340:b5401. doi: 10.1136/bmj.b5401. BMJ. 2010. PMID: 20083544 No abstract available.
References
-
- Landesberg G, Shatz V, Akopnik I, Wolf YG, Mayer M, Berlatzky Y, et al. Association of cardiac troponin, CK-MB, and postoperative myocardial ischemia with long-term survival after major vascular surgery. J Am Coll Cardiol 2003;42:1547-54. - PubMed
-
- Fleischmann KE, Goldman L, Young B, Lee TH. Association between cardiac and noncardiac complications in patients undergoing noncardiac surgery: outcomes and effects on length of stay. Am J Med 2003;115:515-20. - PubMed
-
- Poldermans D, Boersma E, Bax JJ, Thomson IR, van de Ven LLM, Blankensteijn JD, et al. The effect of bisoprolol on perioperative mortality and myocardial infarction in high-risk patients undergoing vascular surgery. N Engl J Med 1999;341:1789-94. - PubMed
-
- Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof E, Fleischmann KE, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery): developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. Circulation 2007;116:e418-99.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous