

Thoracic CT findings of novel influenza A (H1N1) infection in immunocompromised patients
- PMID: 20111882
- PMCID: PMC2880241
- DOI: 10.1007/s10140-010-0859-x
Thoracic CT findings of novel influenza A (H1N1) infection in immunocompromised patients
Abstract
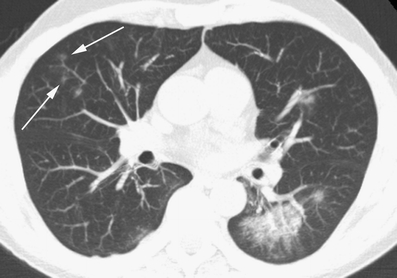
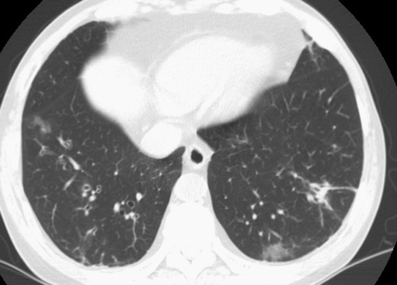
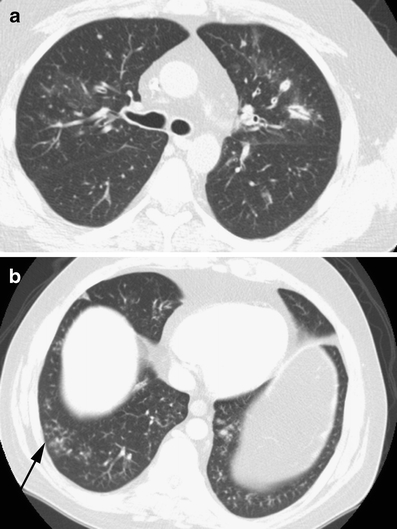
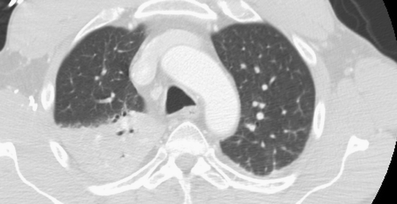
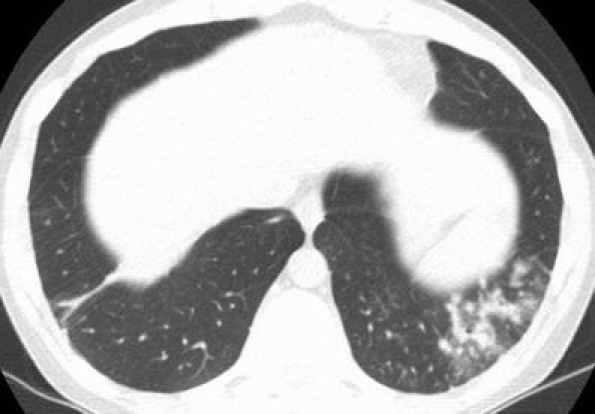
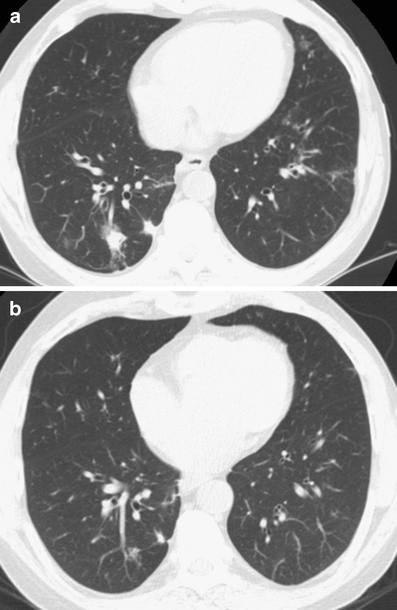
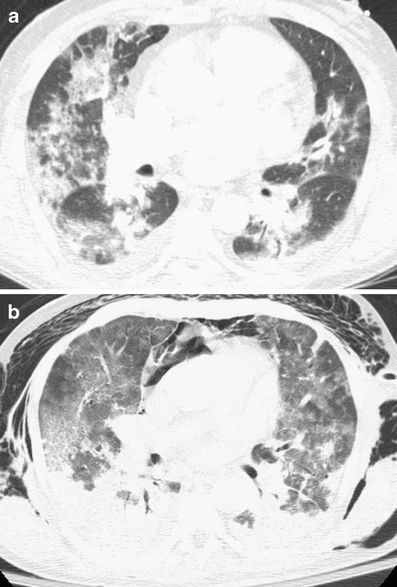
The goal of this study is to describe the spectrum of initial and follow-up CT findings of novel influenza A (H1N1) infection in a series of immunocompromised patients. Eight immunocompromised patients with documented novel influenza A (H1N1) had CT imaging at our institution between May 2009 and August 2009. A total of 20 CTs (initial and follow-up) were reviewed for the presence, severity, and distribution of the following: ground glass opacity, consolidation, interlobular septal thickening, mosaic perfusion, airway wall thickening, airway dilatation, nodules, cysts, pleural effusion, pericardial effusion, lymphadenopathy, and air trapping. The most common findings were airway thickening/dilatation, peribronchial ground glass opacity, centrilobular nodules, and tree-in-bud opacities. Peripheral consolidation involving the lower lobes was also a common pattern. Findings frequently involved all lobes and were closely associated with either large or small airways. Two patients presented with atypical CT findings including focal lobar consolidation and patchy lower lobe consolidation with soft tissue centrilobular nodules. Most survivors showed near complete resolution of findings within 35 days. CT scans in immunocompromised patients with novel influenza H1N1 commonly show a strong airway predominance of findings or peripheral areas of consolidation involving the lower lobes. A subset of patients with novel influenza A (H1N1) will show findings not typical of viral infection.
Figures

Similar articles
-
Novel influenza A (H1N1) virus infection in children: chest radiographic and CT evaluation.Korean J Radiol. 2010 Nov-Dec;11(6):656-64. doi: 10.3348/kjr.2010.11.6.656. Epub 2010 Oct 29. Korean J Radiol. 2010. PMID: 21076592 Free PMC article.
-
64 multidetector CT findings of influenza A (H1N1) virus in patients with hematologic malignancies.Acta Radiol. 2012 Jul;53(6):662-7. doi: 10.1258/ar.2012.120038. Epub 2012 Jun 25. Acta Radiol. 2012. PMID: 22734081
-
Swine-origin influenza A viral (H1N1) infection in children: chest computed tomography findings.Jpn J Radiol. 2011 Dec;29(10):707-11. doi: 10.1007/s11604-011-0619-1. Epub 2011 Oct 19. Jpn J Radiol. 2011. PMID: 22009422
-
Swine-origin influenza A (H1N1) viral infection: thoracic findings on CT.AJR Am J Roentgenol. 2011 Jun;196(6):W723-8. doi: 10.2214/AJR.10.5109. AJR Am J Roentgenol. 2011. PMID: 21606260 Review.
-
CT signs and patterns of lung disease.Radiol Clin North Am. 2001 Nov;39(6):1115-35. doi: 10.1016/s0033-8389(05)70334-1. Radiol Clin North Am. 2001. PMID: 11699664 Review.
Cited by
-
Chest Computed Tomography Findings in COVID-19 and Influenza: A Narrative Review.Biomed Res Int. 2020 Jun 5;2020:6928368. doi: 10.1155/2020/6928368. eCollection 2020. Biomed Res Int. 2020. PMID: 32596354 Free PMC article. Review.
-
Vital role of chest CT in diagnosis of coronavirus disease 2019 (COVID-19).Caspian J Intern Med. 2020 May;11(3):244-249. doi: 10.22088/cjim.11.3.244. Caspian J Intern Med. 2020. PMID: 32874430 Free PMC article. Review.
-
High-resolution computed tomography findings of influenza virus pneumonia: a comparative study between seasonal and novel (H1N1) influenza virus pneumonia.Jpn J Radiol. 2012 Feb;30(2):154-61. doi: 10.1007/s11604-011-0027-6. Epub 2011 Dec 17. Jpn J Radiol. 2012. PMID: 22180185
-
Community acquired respiratory virus infections in cancer patients-Guideline on diagnosis and management by the Infectious Diseases Working Party of the German Society for haematology and Medical Oncology.Eur J Cancer. 2016 Nov;67:200-212. doi: 10.1016/j.ejca.2016.08.015. Epub 2016 Sep 25. Eur J Cancer. 2016. PMID: 27681877 Free PMC article. Review.
-
Pulmonary High-Resolution Computed Tomography (HRCT) Findings of Patients with Early-Stage Coronavirus Disease 2019 (COVID-19) in Hangzhou, China.Med Sci Monit. 2020 Apr 4;26:e923885. doi: 10.12659/MSM.923885. Med Sci Monit. 2020. PMID: 32246819 Free PMC article.
References
-
- World Health Organization. Pandemic (H1N1) 2009—update 71. http://www.who.int/csr/don/2009_10_23/en/index.html. Accessed October 26, 2009
