

The treatment of Barrett's esophagus
- PMID: 20112466
- PMCID: PMC5052494
The treatment of Barrett's esophagus
Abstract
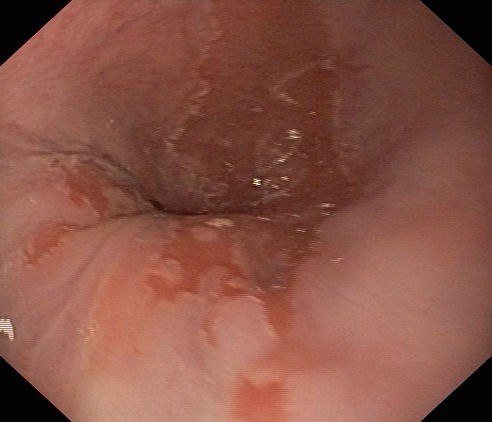
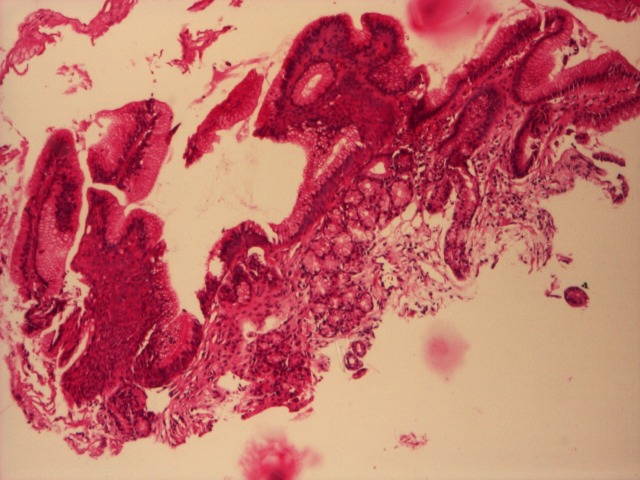
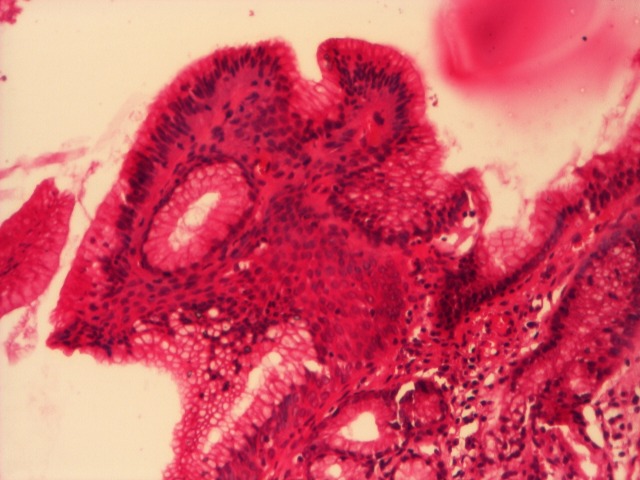
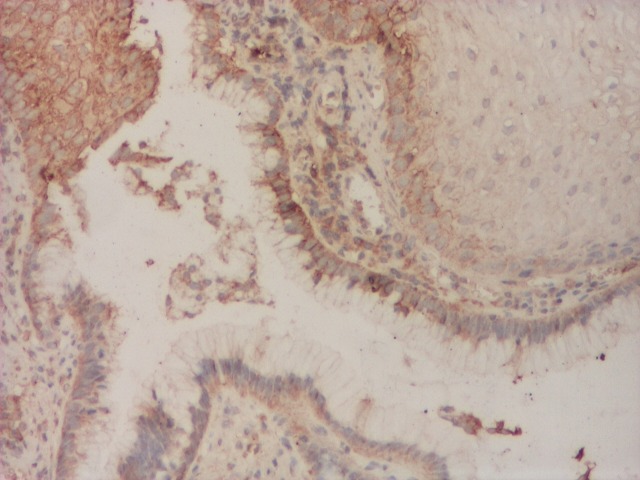
The reflux of the gastric juice in the esophagus can determine the injury of the esophageal epithelium. When the healing of the lesion is done by replacing the normal squamous epithelium with columnar epithelium, the entity is called Barrett's esophagus (BE). Although controversial, some studies showed 0,5% per year the incidence of the esophageal adenocarcinoma in patients with BE, 30 times more often than general population. Taking into consideration the possible development of an adenocarcinoma, the patients with Barrett's esophagus require endoscopic surveillance after a standardized protocol. There is still much controversy about the treatment of patients with Barrett's esophagus, especially in the presence of dysplasia. The aims of the treatment are gastro-esophageal reflux symptoms control, healing of associated esophagitis and prevention of development of adenocarcinoma.
Figures

Similar articles
-
Management of Barrett's esophagus.Mayo Clin Proc. 1998 May;73(5):457-61. doi: 10.1016/S0025-6196(11)63730-0. Mayo Clin Proc. 1998. PMID: 9581588 Review.
-
Barrett's esophagus and esophageal adenocarcinoma: pathogenesis, diagnosis, and therapy.Med Clin North Am. 2002 Nov;86(6):1423-45, vii. doi: 10.1016/s0025-7125(02)00082-2. Med Clin North Am. 2002. PMID: 12510459 Review.
-
Management strategies of Barrett's esophagus.World J Gastroenterol. 2012 Nov 21;18(43):6216-25. doi: 10.3748/wjg.v18.i43.6216. World J Gastroenterol. 2012. PMID: 23180941 Free PMC article. Review.
-
Barrett's oesophagus: Current controversies.World J Gastroenterol. 2017 Jul 28;23(28):5051-5067. doi: 10.3748/wjg.v23.i28.5051. World J Gastroenterol. 2017. PMID: 28811703 Free PMC article. Review.
-
The columnar-lined (Barrett's) esophagus. Can progression to cancer be prevented?Postgrad Med. 2000 Jun;107(7):59-65; quiz 216. doi: 10.3810/pgm.2000.06.1125. Postgrad Med. 2000. PMID: 10887445 Review.
Cited by
-
Radical excision of Barrett's esophagus and complete recovery of normal squamous epithelium.World J Gastroenterol. 2013 Aug 21;19(31):5195-8. doi: 10.3748/wjg.v19.i31.5195. World J Gastroenterol. 2013. PMID: 23964158 Free PMC article.
-
Surveillance in Barrett esophagus.J Med Life. 2014;7 Spec No. 3(Spec Iss 3):61-7. J Med Life. 2014. PMID: 25870698 Free PMC article.
References
-
- Shaheen N.J., Crosby M.A., Bozymski E.M., Sandler R.S. Is there publication bias in the reporting of cancer risk in Barrett’s esophagus? Gastroenterology. 2000;119:333–338. - PubMed
-
- Westhoff B, Brotze S, Weston A, et al. The frequency of Barrett’s esophagus in high-risk patients with chronic GERD. Gastrointest Endosc. 2005;61:226 –231. - PubMed
-
- Ioan Nicolae Mates. Diversia duodenala in patologia de reflux. Bucuresti: Ed Universitara “Carol Davila”; 2008.
-
- Yeh R.W., Triadafilopoulos G. Endoscopic Therapy for Barrett's Esophagus. Gastrointest Endosc Clin N Am. 2005;15(3):377 –397. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources