

Pharmacotherapy in pulmonary arterial hypertension: a systematic review and meta-analysis
- PMID: 20113497
- PMCID: PMC2835653
- DOI: 10.1186/1465-9921-11-12
Pharmacotherapy in pulmonary arterial hypertension: a systematic review and meta-analysis
Abstract
Background: Previous meta-analyses of treatments for pulmonary arterial hypertension (PAH) have not shown mortality benefit from any individual class of medication.
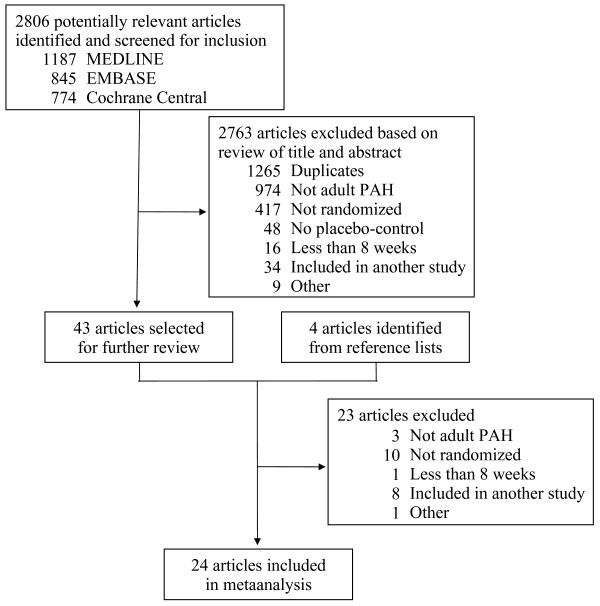
Methods: MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials were searched from inception through November 2009 for randomized trials that evaluated any pharmacotherapy in the treatment of PAH. Reference lists from included articles and recent review articles were also searched. Analysis included randomized placebo controlled trials of at least eight weeks duration and studies comparing intravenous medication to an unblinded control group.
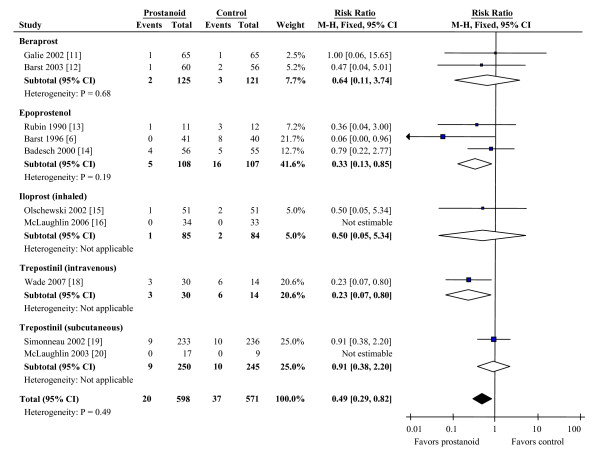
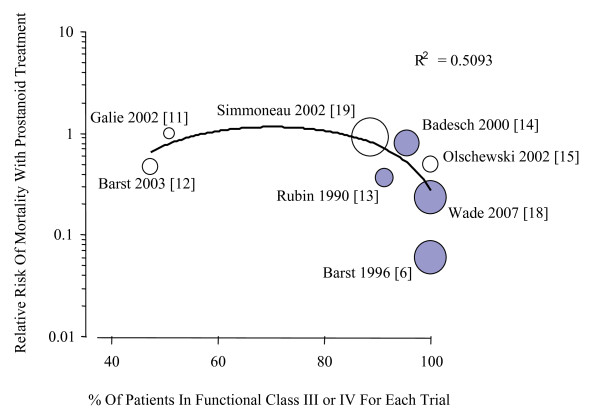
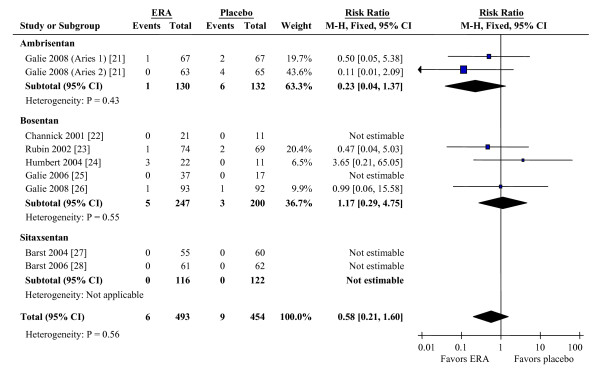
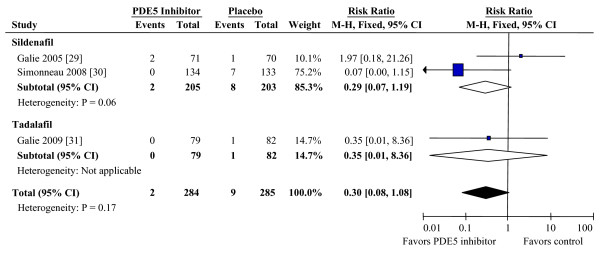
Results: 1541 unique studies were identified and twenty-four articles with 3758 patients were included in the meta-analysis. Studies were reviewed and data extracted regarding study characteristics and outcomes. Data was pooled for three classes of medication: prostanoids, endothelin-receptor antagonists (ERAs), and phosphodiesterase type 5 (PDE5) inhibitors. Pooled relative risks (RRs) and 95% confidence intervals (CIs) were calculated for mortality, 6-minute walk distance, dyspnea scores, hemodynamic parameters, and adverse effects. Mortality in the control arms was a combined 4.2% over the mean study length of 14.9 weeks. There was significant mortality benefit with prostanoid treatment (RR 0.49, CI 0.29 to 0.82), particularly comparing intravenous agents to control (RR 0.30, CI 0.14 to 0.63). Mortality benefit was not observed for ERAs (RR 0.58, CI 0.21 to 1.60) or PDE5 inhibitors (RR 0.30, CI 0.08 to 1.08). All three classes of medication improved other clinical and hemodynamic endpoints. Adverse effects that were increased in treatment arms include jaw pain, diarrhea, peripheral edema, headache, and nausea in prostanoids; and visual disturbance, dyspepsia, flushing, headache, and limb pain in PDE5 inhibitors. No adverse events were significantly associated with ERA treatment.
Conclusions: Treatment of PAH with prostanoids reduces mortality and improves multiple other clinical and hemodynamic outcomes. ERAs and PDE5 inhibitors improve clinical and hemodynamic outcomes, but have no proven effect on mortality. The long-term effects of all PAH treatment requires further study.
Figures
References
-
- Voelkel NF, Tuder RM, Weir EK, Rubin L, Rich S. Primary Pulmonary Hypertension. New York, NY: Marcel Dekker; 1997. Pathophysiology of primary pulmonary hypertension; pp. 83–129.
-
- Voelkel NF, Quaife RA, Leinwand LA, Barst RJ, McGoon MD, Meldrum DR, Dupuis J, Long CS, Rubin LJ, Smart FW, Suzuki YJ, Gladwin M, Denholm EM, Gail DB. National Heart, Lung, and Blood Institute Working Group on Cellular and Molecular Mechanisms of Right Heart Failure. Right ventricular function and failure: report of a National Heart, Lung, and Blood Institute working group on cellular and molecular mechanisms of right heart failure. Circulation. 2006;114:1883–1891. doi: 10.1161/CIRCULATIONAHA.106.632208. - DOI - PubMed
-
- D'Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, Fishman AP, Goldring RM, Groves BM, Kernis JT. et al.Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. 1991;115:343–349. - PubMed
-
- McLaughlin VV, Archer SL, Badesch DB, Barst RJ, Farber HW, Lindner JR, Mathier MA, McGoon MD, Park MH, Rosenson RS, Rubin LJ, Tapson VF, Varga J, Harrington RA, Anderson JL, Bates ER, Bridges CR, Eisenberg MJ, Ferrari VA, Grines CL, Hlatky MA, Jacobs AK, Kaul S, Lichtenberg RC, Lindner JR, Moliterno DJ, Mukherjee D, Pohost GM, Rosenson RS, Schofield RS, Shubrooks SJ, Stein JH, Tracy CM, Weitz HH, Wesley DJ. ACCF/AHA. ACCF/AHA 2009 expert consensus document on pulmonary hypertension: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association: developed in collaboration with the American College of Chest Physicians, American Thoracic Society, Inc., and the Pulmonary Hypertension Association. Circulation. 2009;119:2250–2294. doi: 10.1161/CIRCULATIONAHA.109.192230. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
