

Risk factors for and estimated incidence of community-associated Clostridium difficile infection, North Carolina, USA
- PMID: 20113547
- PMCID: PMC2958012
- DOI: 10.3201/eid1602.090953
Risk factors for and estimated incidence of community-associated Clostridium difficile infection, North Carolina, USA
Abstract
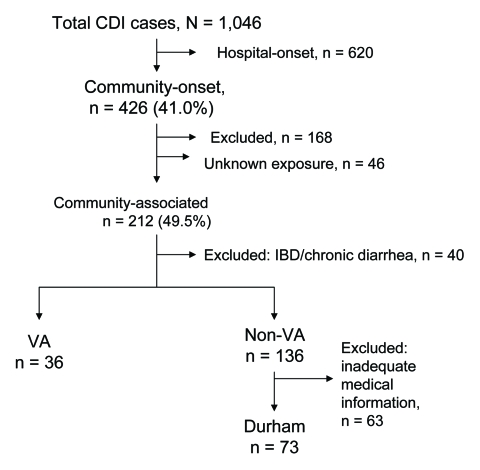
We determined estimated incidence of and risk factors for community-associated Clostridium difficile infection (CA-CDI) among patients treated at 6 North Carolina hospitals. CA-CDI case-patients were defined as adults (>18 years of age) with a positive stool test result for C. difficile toxin and no hospitalization within the prior 8 weeks. CA-CDI incidence was 21 and 46 per 100,000 person-years in Veterans Affairs (VA) outpatients and Durham County populations, respectively. VA case-patients were more likely than controls to have received antimicrobial drugs (adjusted odds ratio [aOR] 17.8, 95% confidence interval [CI] 6.6-48] and to have had a recent outpatient visit (aOR 5.1, 95% CI 1.5-17.9). County case-patients were more likely than controls to have received antimicrobial drugs (aOR 9.1, 95% CI 2.9-28.9), to have gastroesophageal reflux disease (aOR 11.2, 95% CI 1.9-64.2), and to have cardiac failure (aOR 3.8, 95% CI 1.1-13.7). Risk factors for CA-CDI overlap with those for healthcare-associated infection.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources