

Hydroxyurea for children with sickle cell disease
- PMID: 20113903
- PMCID: PMC4765496
- DOI: 10.1016/j.hoc.2009.11.002
Hydroxyurea for children with sickle cell disease
Abstract
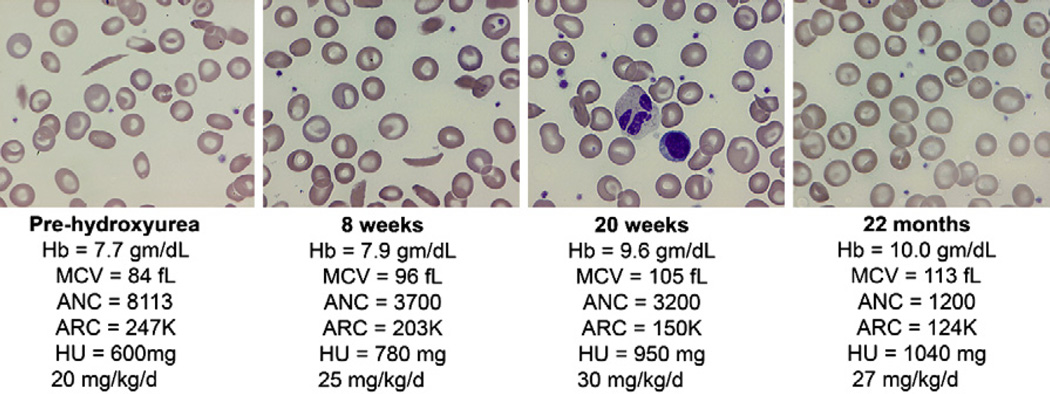
Hydroxyurea therapy offers promise for ameliorating the clinical course of children with sickle cell disease (SCD). Hydroxyurea is a prototypic therapeutic option; it can be administered with minimal side effects, has a relatively wide therapeutic window, and has mechanisms of action that address pathophysiologic pathways of sickling, vaso-occlusion, hemolysis, and organ damage. There are limited data regarding hydroxyurea's ability to prevent or diminish organ dysfunction, and the long-term risks of hydroxyurea therapy remain incompletely defined. Although clinical trials are underway to address long-term issues, hydroxyurea remains an effective but underutilized therapy for SCD.
Copyright (c) 2010 Elsevier Inc. All rights reserved.
Figures

Similar articles
-
Hydroxyurea for children with sickle cell disease.Pediatr Clin North Am. 2008 Apr;55(2):483-501, x. doi: 10.1016/j.pcl.2008.02.003. Pediatr Clin North Am. 2008. PMID: 18381097 Review.
-
Hydroxyurea therapy in children severely affected with sickle cell disease.J Pediatr. 1996 Jun;128(6):820-8. doi: 10.1016/s0022-3476(96)70335-9. J Pediatr. 1996. PMID: 8648542
-
Hydroxyurea therapy: improving the lives of patients with sickle cell disease.Pediatr Nurs. 2006 Nov-Dec;32(6):541-3. Pediatr Nurs. 2006. PMID: 17256291 Review.
-
Long-term hydroxyurea treatment in children with sickle cell disease: tolerance and clinical outcomes.Haematologica. 2006 Jan;91(1):125-8. Haematologica. 2006. PMID: 16434381 Clinical Trial.
-
Hydroxyurea and sickle cell anemia. Clinical utility of a myelosuppressive "switching" agent. The Multicenter Study of Hydroxyurea in Sickle Cell Anemia.Medicine (Baltimore). 1996 Nov;75(6):300-26. doi: 10.1097/00005792-199611000-00002. Medicine (Baltimore). 1996. PMID: 8982148 Clinical Trial.
Cited by
-
Utilization of Hydroxyurea Among Patients Diagnosed with Sickle Cell Disease in Jazan, Saudi Arabia.Patient Prefer Adherence. 2022 Nov 8;16:3059-3067. doi: 10.2147/PPA.S390568. eCollection 2022. Patient Prefer Adherence. 2022. PMID: 36387052 Free PMC article.
-
The role of hydroxyurea in decreasing the occurrence of vasso-occulusive crisis in pediatric patients with sickle cell disease at King Saud Medical City in Riyadh, Saudi Arabia.Saudi Med J. 2020 Jan;41(1):46-52. doi: 10.15537/smj.2020.1.24698. Saudi Med J. 2020. PMID: 31915794 Free PMC article.
-
Hydroxyurea use and hospitalization trends in a comprehensive pediatric sickle cell program.PLoS One. 2013 Aug 14;8(8):e72077. doi: 10.1371/journal.pone.0072077. eCollection 2013. PLoS One. 2013. PMID: 23967276 Free PMC article.
-
Hydroxyurea and Zileuton Differentially Modulate Cell Proliferation and Interleukin-2 Secretion by Murine Spleen Cells: Possible Implication on the Immune Function and Risk of Pain Crisis in Patients with Sickle Cell Disease.Ochsner J. 2015 Fall;15(3):241-7. Ochsner J. 2015. PMID: 26412995 Free PMC article.
-
Post-Transcriptional Genetic Silencing of BCL11A to Treat Sickle Cell Disease.N Engl J Med. 2021 Jan 21;384(3):205-215. doi: 10.1056/NEJMoa2029392. Epub 2020 Dec 5. N Engl J Med. 2021. PMID: 33283990 Free PMC article. Clinical Trial.
References
-
- Platt OS, Thorington BD, Brambilla DJ, et al. Pain in sickle cell disease. Rates and risk factors. N Engl J Med. 1991;325(1):11–16. - PubMed
-
- Steinberg MH, Rosenstock W, Coleman MB, et al. Effects of thalassemia and microcytosis on the hematologic and vasoocclusive severity of sickle cell anemia. Blood. 1984;63(6):1353–1360. - PubMed
-
- Baum KF, Dunn DT, Maude GH, et al. The painful crisis of homozygous sickle cell disease. A study of the risk factors. Arch Intern Med. 1987;147(7):1231–1234. - PubMed
-
- Phillips G, Jr, Coffey B, Tran-Son-Tay R, et al. Relationship of clinical severity to packed cell rheology in sickle cell anemia. Blood. 1991;78(10):2735–2739. - PubMed
-
- Powars DR. Sickle cell anemia: beta s-gene-cluster haplotypes as prognostic indicators of vital organ failure. Semin Hematol. 1991;28(3):202–208. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
