

Pulsatile left ventricular assist device support as a bridge to decision in patients with end-stage heart failure complicated by pulmonary hypertension
- PMID: 20113910
- PMCID: PMC3066206
- DOI: 10.1016/j.healun.2009.09.013
Pulsatile left ventricular assist device support as a bridge to decision in patients with end-stage heart failure complicated by pulmonary hypertension
Abstract
Background: Severe pulmonary hypertension (PH) in heart failure (HF) is a risk factor for adverse outcomes after heart transplantation (HTx). Left ventricular assist devices (LVADs) improve pulmonary hemodynamics, but our understanding of the degree of improvement and the effect on outcomes is still evolving.
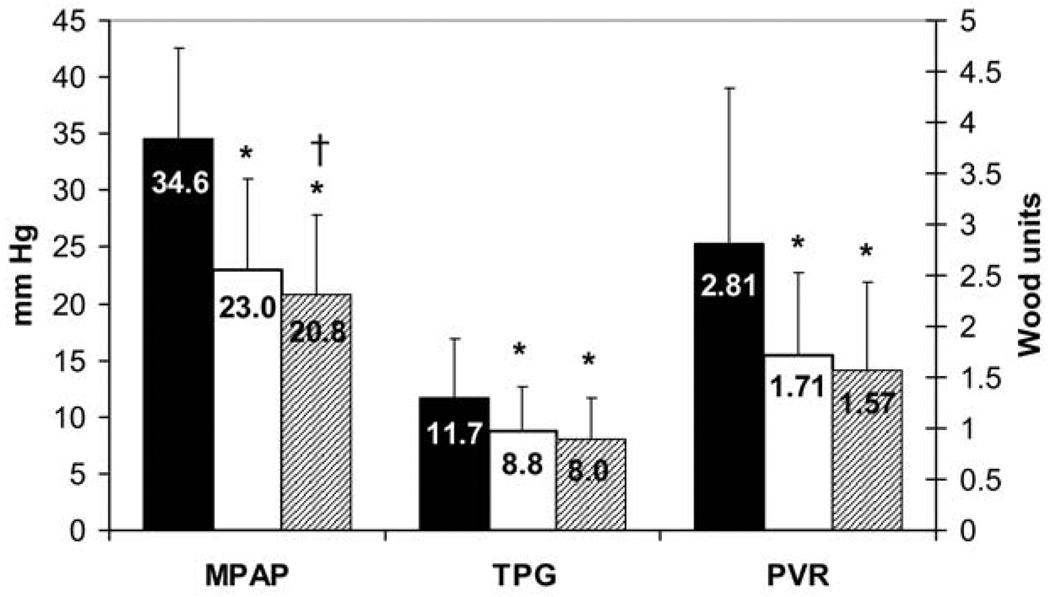
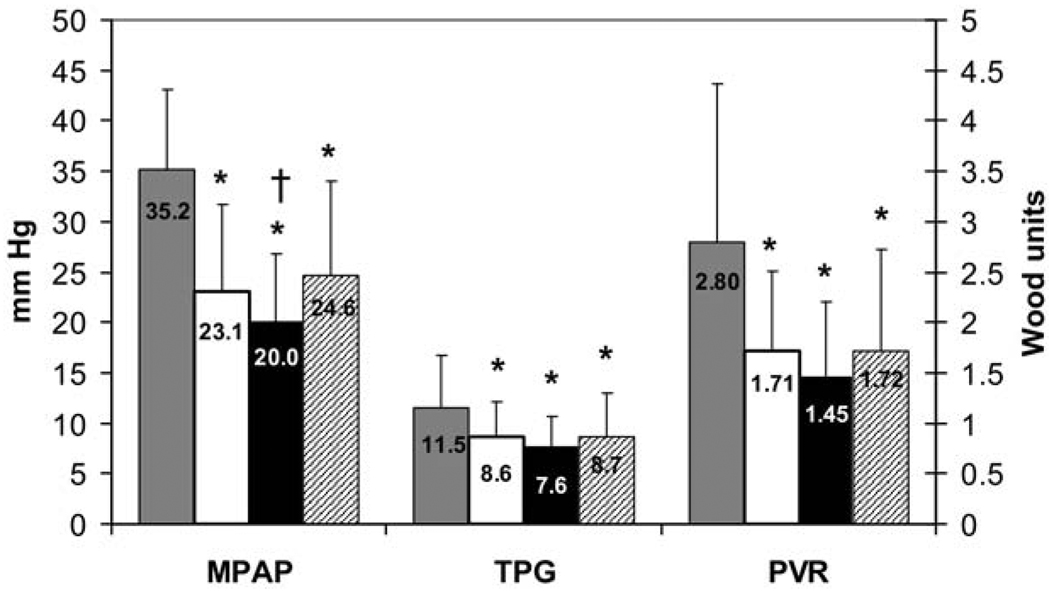
Methods: We reviewed invasive pulmonary hemodynamics from 58 consecutive patients receiving LVAD support as a bridge to HTx from 1996 to 2003. The primary outcome was change in baseline transpulmonary gradient (TPG) during LVAD support and after HTx/recovery. The secondary outcome was post-HTx survival.
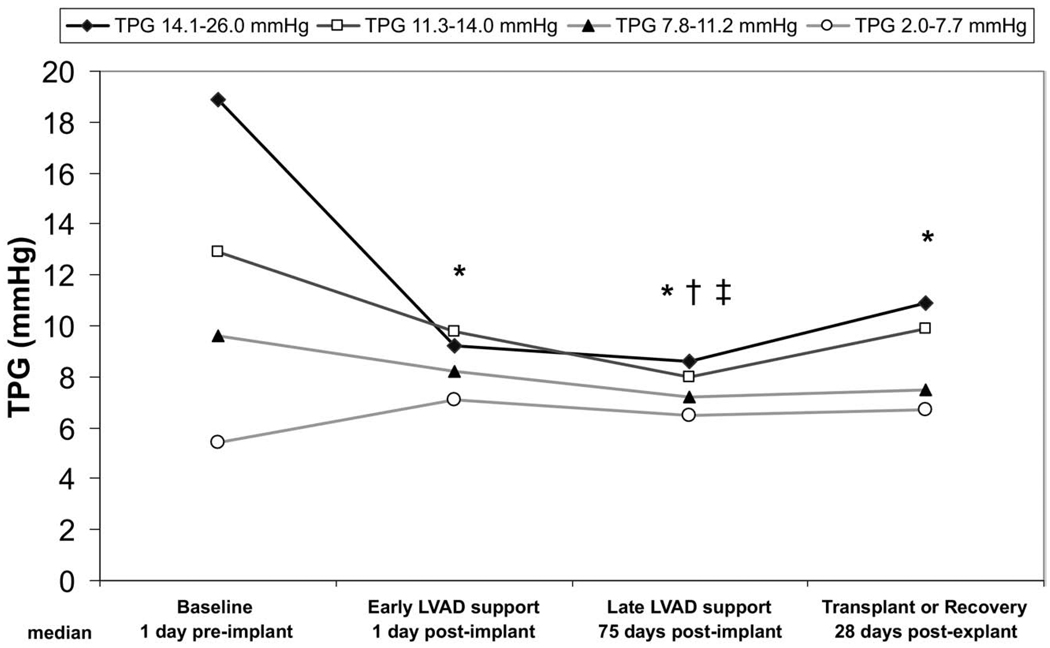
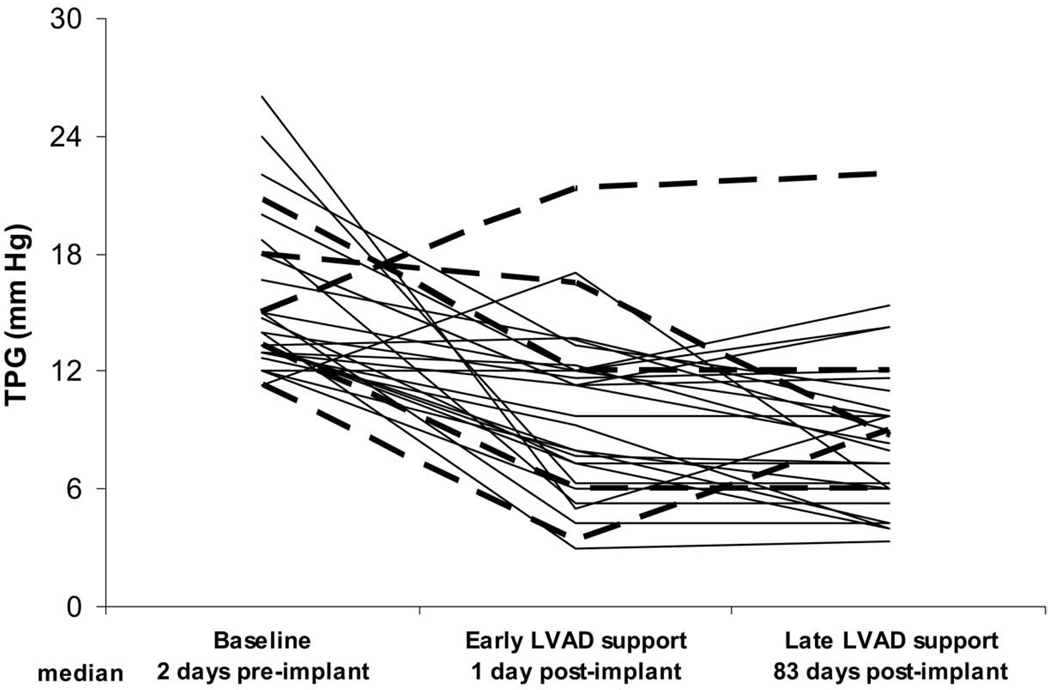
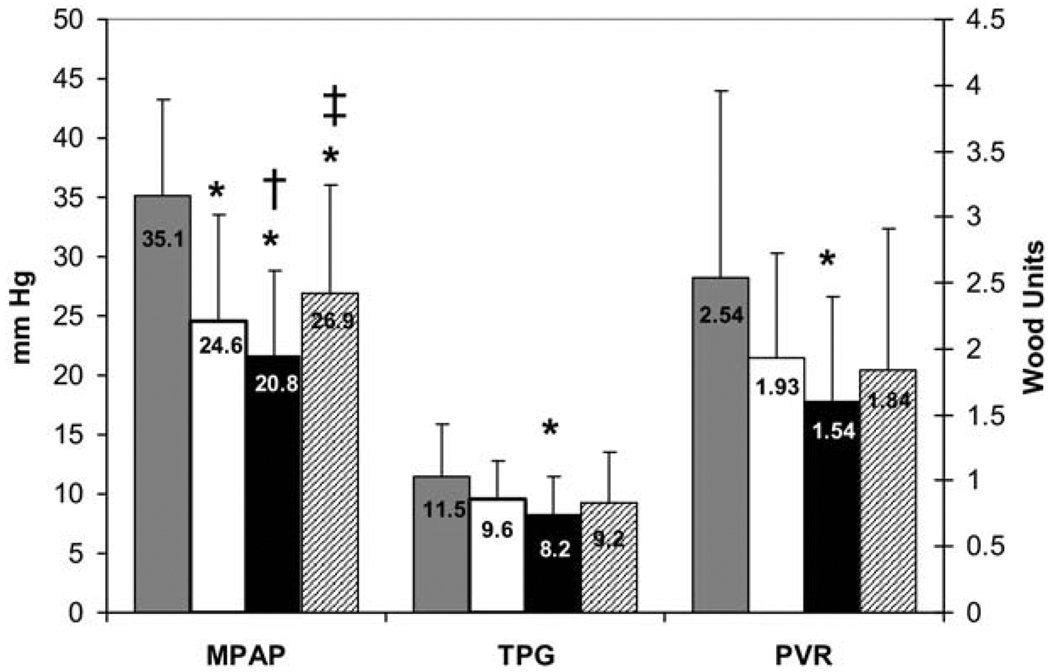
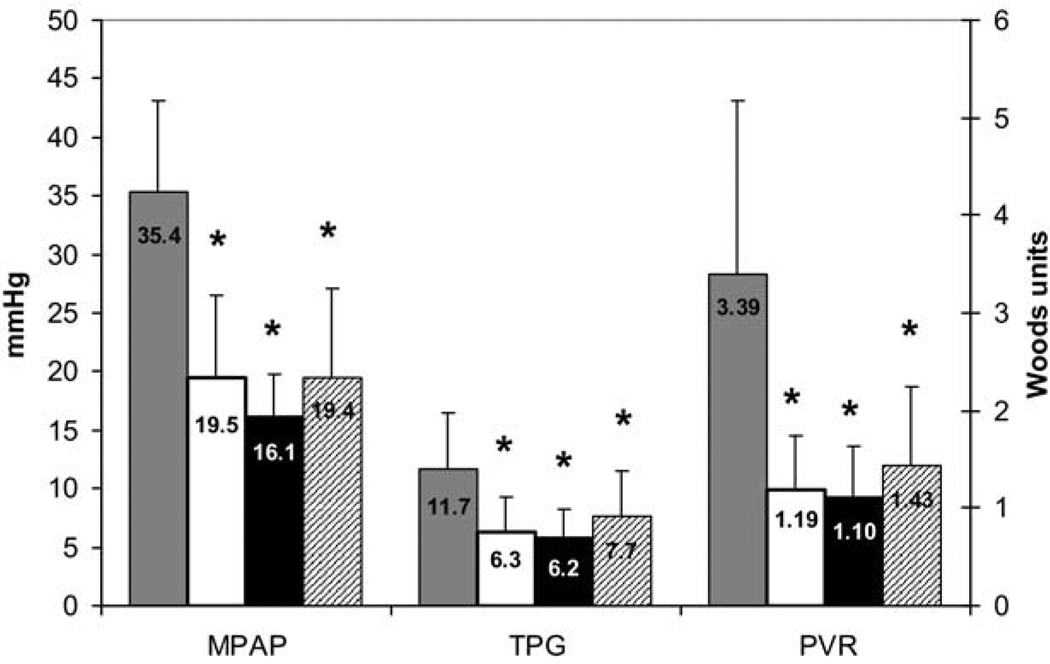
Results: All patients (age, 49 +/- 14 years, 79% male, 40% ischemic) received a pulsatile LVAD (median support, 97 days; interquartile range [IQR], 31-222). Hemodynamic measurements were obtained at baseline (median, 1 day; IQR, 1-3), during early (median, 1 day; IQR, 0-4) and late (median, 75 days; IQR, 24-186) LVAD support, and after HTx/recovery (median, 28 days; IQR, 17-40). Improvement in TPG occurred throughout LVAD support and was sustained after HTx/recovery. Levels of TPG reductions in patients with a baseline TPG in the highest quartile (14.1-26.0 mm Hg) were 8.6 +/- 3.5 vs 6.5 +/- 3.1 mm Hg in the lowest quartile (2.0-7.7 mm Hg) during LVAD support (p = 0.102), with 90% vs 100% 30-day post-HTx survival (P = 0.113).
Conclusion: Pulmonary hemodynamics and post-HTx survival were similar after pulsatile LVAD support in patients with and without pre-implant PH. LVAD support may be a useful strategy to reverse PH in carefully selected patients, thus improving candidacy for HTx.
Conflict of interest statement
None of the other authors has a financial relationship with a commercial entity that has an interest in the subject of the presented manuscript or other conflicts of interest to disclose.
Figures
Comment in
-
Use of a novel short-term mechanical circulatory support device for cardiac recovery.J Heart Lung Transplant. 2011 Jun;30(6):732-3. doi: 10.1016/j.healun.2011.01.725. Epub 2011 Apr 8. J Heart Lung Transplant. 2011. PMID: 21482147 No abstract available.
Similar articles
-
High Transpulmonary Artery Gradient Obtained at the Time of Left Ventricular Assist Device Implantation Negatively Affects Survival After Cardiac Transplantation.J Card Fail. 2019 Oct;25(10):777-784. doi: 10.1016/j.cardfail.2019.03.010. Epub 2019 Mar 20. J Card Fail. 2019. PMID: 30904557 Clinical Trial.
-
Long-term heart transplant outcomes after lowering fixed pulmonary hypertension using left ventricular assist devices.Eur J Cardiothorac Surg. 2018 Dec 1;54(6):1116-1121. doi: 10.1093/ejcts/ezy214. Eur J Cardiothorac Surg. 2018. PMID: 29905775
-
Reversal of secondary pulmonary hypertension by axial and pulsatile mechanical circulatory support.J Heart Lung Transplant. 2010 Feb;29(2):195-200. doi: 10.1016/j.healun.2009.05.030. Epub 2009 Sep 26. J Heart Lung Transplant. 2010. PMID: 19782604
-
Reversibility of fixed pulmonary hypertension in left ventricular assist device support recipients.Eur J Cardiothorac Surg. 2011 Oct;40(4):971-7. doi: 10.1016/j.ejcts.2011.01.019. Epub 2011 Feb 26. Eur J Cardiothorac Surg. 2011. PMID: 21354812 Review.
-
Revisiting Pulmonary Hypertension in the Era of Temporary Mechanical Circulatory Support - Literature Review and Case-Based Discussion.Transplant Proc. 2023 Dec;55(10):2462-2469. doi: 10.1016/j.transproceed.2023.09.022. Epub 2023 Nov 18. Transplant Proc. 2023. PMID: 37980253 Review.
Cited by
-
Saudi Guidelines on the Diagnosis and Treatment of Pulmonary Hypertension: Pulmonary hypertension due to left heart disease.Ann Thorac Med. 2014 Jul;9(Suppl 1):S47-55. doi: 10.4103/1817-1737.134026. Ann Thorac Med. 2014. PMID: 25076997 Free PMC article.
-
Right heart failure after left ventricular assist device: From mechanisms to treatments.Front Cardiovasc Med. 2022 Oct 19;9:1023549. doi: 10.3389/fcvm.2022.1023549. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36337897 Free PMC article. Review.
-
Torrential Mitral Regurgitation After Transcatheter Edge-to-Edge Mitral Valve Repair.JACC Case Rep. 2021 Jan 20;3(1):69-73. doi: 10.1016/j.jaccas.2020.11.039. eCollection 2021 Jan. JACC Case Rep. 2021. PMID: 34317471 Free PMC article.
-
Early reduction of pulmonary arterial hypertension in patients using a long-term mechanical ventricular assistance device: a cross-sectional study.Sao Paulo Med J. 2022 May-Jun;140(3):505-508. doi: 10.1590/1516-3180.2021.0944.R2.18032022. Sao Paulo Med J. 2022. PMID: 35584527 Free PMC article.
-
Simulation of dilated heart failure with continuous flow circulatory support.PLoS One. 2014 Jan 17;9(1):e85234. doi: 10.1371/journal.pone.0085234. eCollection 2014. PLoS One. 2014. PMID: 24465511 Free PMC article.
References
-
- Massad MG. Surgical options for the management of congestive heart failure. Cardiology. 2004;101:5–6. - PubMed
-
- Taylor DO, Edwards LB, Boucek MM, Trulock EP, Keck BM, Hertz MI. The registry of the International Society for Heart and Lung Transplantation: twenty-first official adult heart transplant report—2004. J Heart Lung Transplant. 2004;23:796–803. - PubMed
-
- Constanzo MR, Augustine S, Bouge R, et al. Selection and treatment of candidates for heart transplantation. A statement for health professionals from the committee on heart failure and cardiac transplantation of the council on clinical cardiology, American Heart Association. Circulation. 1995;92:3593–3612. - PubMed
-
- Mehra MR, Kobashigawa J, Starling R, et al. Listing criteria for heart transplantation: International Society for Heart and Lung Transplantation guidelines for the care of cardiac transplant candidates—2006. J Heart Lung Transplant. 2006;25:1024–1042. - PubMed
-
- Kirklin JK, Naftel DC, Kirklin JW, Blackstone EH, White-Williams C, Bourge RC. Pulmonary vascular resistance and the risk of heart transplantation. J Heart Transplant. 1988;7:331–336. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
