

Dynamic cardiovascular risk assessment in elderly people. The role of repeated N-terminal pro-B-type natriuretic peptide testing
- PMID: 20117457
- PMCID: PMC2840257
- DOI: 10.1016/j.jacc.2009.07.069
Dynamic cardiovascular risk assessment in elderly people. The role of repeated N-terminal pro-B-type natriuretic peptide testing
Abstract
Objectives: This study sought to determine whether serial measurement of N-terminal pro-B-type natriuretic peptide (NT-proBNP) in community-dwelling elderly people would provide additional prognostic information to that from traditional risk factors.
Background: Accurate cardiovascular risk stratification is challenging in elderly people.
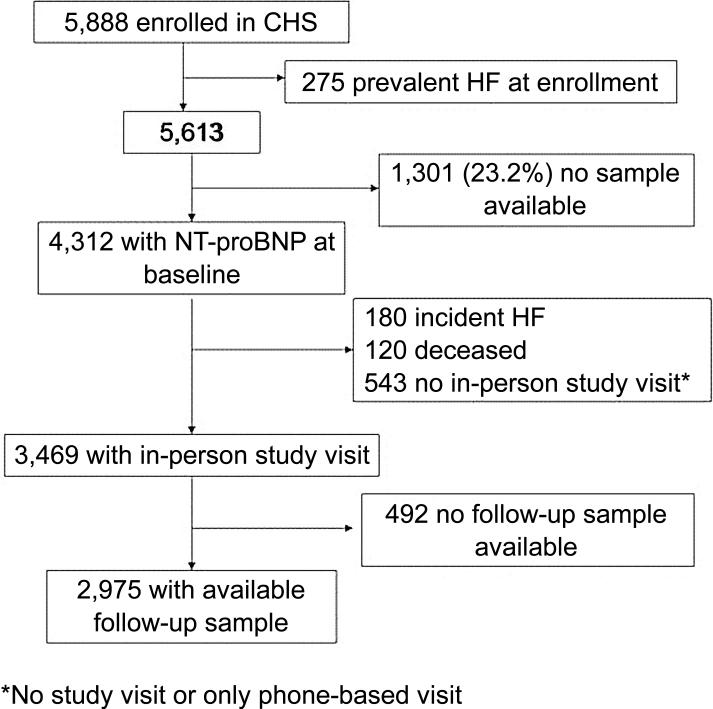
Methods: NT-proBNP was measured at baseline and 2 to 3 years later in 2,975 community-dwelling older adults free of heart failure in the longitudinal CHS (Cardiovascular Health Study). This investigation examined the risk of new-onset heart failure (HF) and death from cardiovascular causes associated with baseline NT-proBNP and changes in NT-proBNP levels, adjusting for potential confounders.
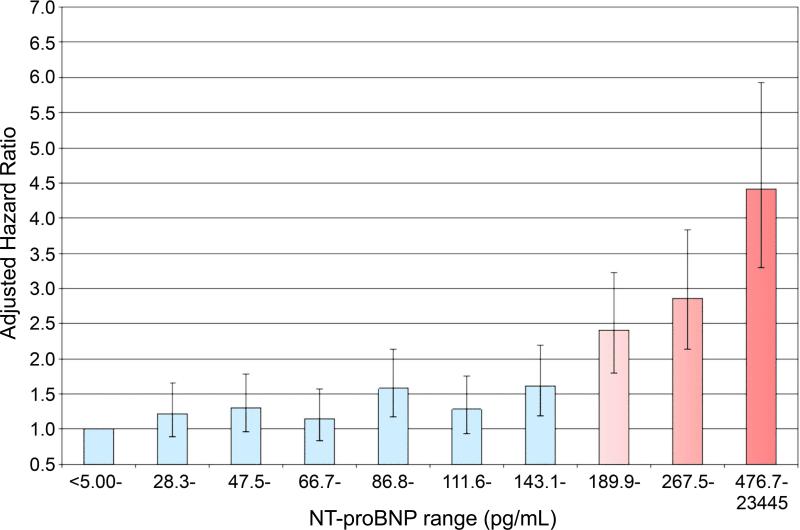
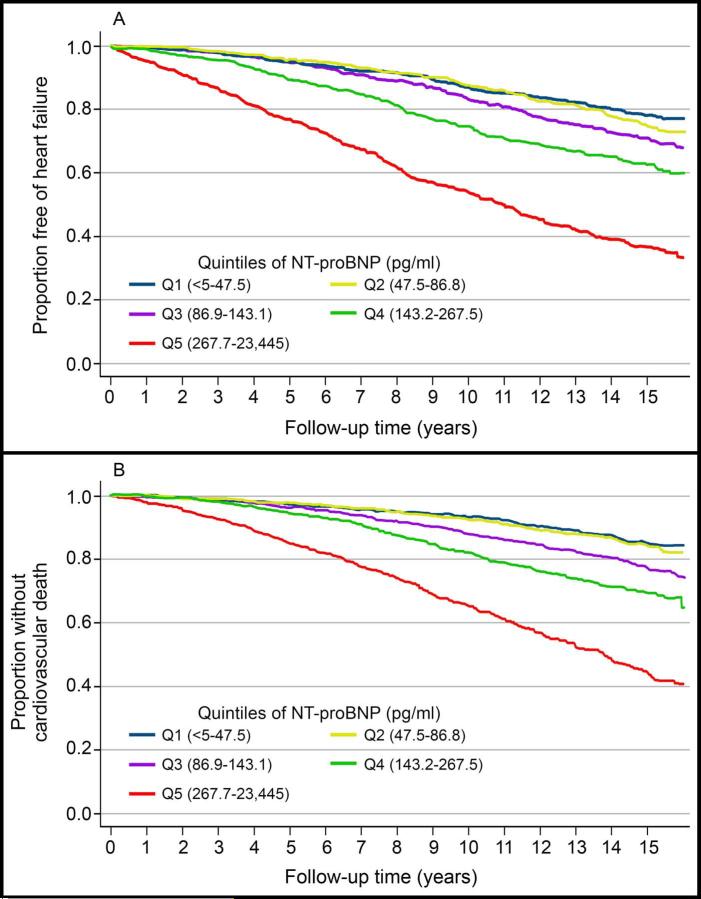
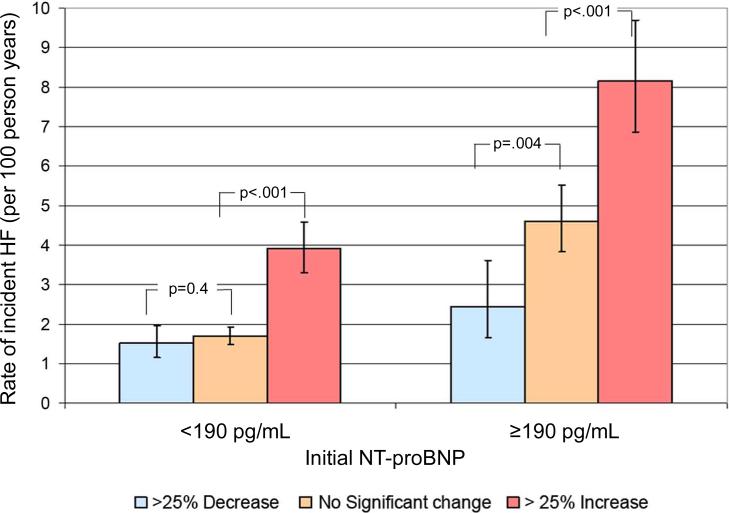
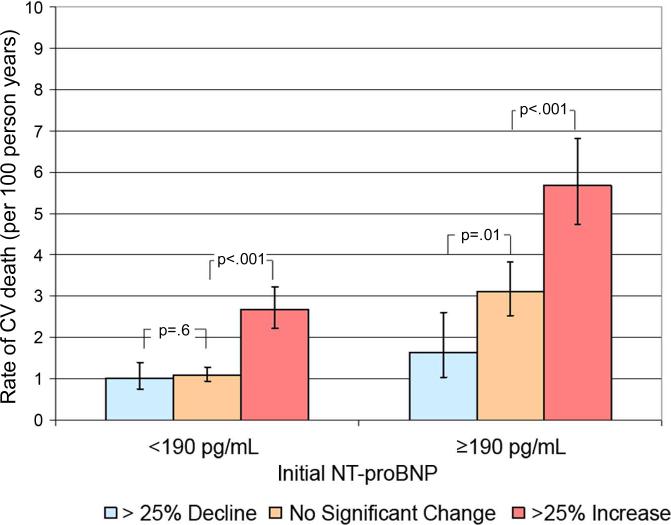
Results: NT-proBNP levels in the highest quintile (>267.7 pg/ml) were independently associated with greater risks of HF (hazard ratio [HR]: 3.05; 95% confidence interval [CI]: 2.46 to 3.78) and cardiovascular death (HR: 3.02; 95% CI: 2.36 to 3.86) compared with the lowest quintile (<47.5 pg/ml). The inflection point for elevated risk occurred at NT-proBNP 190 pg/ml. Among participants with initially low NT-proBNP (<190 pg/ml), those who developed a >25% increase on follow-up to >190 pg/ml (21%) were at greater adjusted risk of HF (HR: 2.13; 95% CI: 1.68 to 2.71) and cardiovascular death (HR: 1.91; 95% CI: 1.43 to 2.53) compared with those with sustained low levels. Among participants with initially high NT-proBNP, those who developed a >25% increase (40%) were at higher risk of HF (HR: 2.06; 95% CI: 1.56 to 2.72) and cardiovascular death (HR: 1.88; 95% CI: 1.37 to 2.57), whereas those who developed a >25% decrease to <or=190 pg/ml (15%) were at lower risk of HF (HR: 0.58; 95% CI: 0.36 to 0.93) and cardiovascular death (HR: 0.57; 95% CI: 0.32 to 1.01) compared with those with unchanged high values.
Conclusions: NT-proBNP levels independently predict heart failure and cardiovascular death in older adults. NT-proBNP levels frequently change over time, and these fluctuations reflect dynamic changes in cardiovascular risk.
Copyright (c) 2010 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Improving risk stratification for heart failure. A role for serial testing of B-type natriuretic peptides?J Am Coll Cardiol. 2010 Feb 2;55(5):451-3. doi: 10.1016/j.jacc.2009.08.060. J Am Coll Cardiol. 2010. PMID: 20117458 No abstract available.
References
-
- Schocken DD, Arrieta MI, Leaverton PE, Ross EA. Prevalence and mortality rate of congestive heart failure in the United States. J Am Coll Cardiol. 1992;20:301–6. - PubMed
-
- Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics--2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115:e69–171. - PubMed
-
- D'Agostino RB, Sr., Grundy S, Sullivan LM, Wilson P. Validation of the Framingham coronary heart disease prediction scores: results of a multiple ethnic groups investigation. Jama. 2001;286:180–7. - PubMed
-
- Kuller LH, Arnold AM, Psaty BM, et al. 10-year follow-up of subclinical cardiovascular disease and risk of coronary heart disease in the Cardiovascular Health Study. Arch Intern Med. 2006;166:71–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 HL075366/HL/NHLBI NIH HHS/United States
- N01-HC-85085/HC/NHLBI NIH HHS/United States
- N01-HC-85081/HC/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- P30-AG-024827/AG/NIA NIH HHS/United States
- N01-HC-85086/HC/NHLBI NIH HHS/United States
- AG-027058/AG/NIA NIH HHS/United States
- N01-HC-85082/HC/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- N01-HC-55222/HC/NHLBI NIH HHS/United States
- R01 AG020098/AG/NIA NIH HHS/United States
- N01-HC-85079/HC/NHLBI NIH HHS/United States
- N01 HC075150/HL/NHLBI NIH HHS/United States
- R01 AG027058/AG/NIA NIH HHS/United States
- N01-HC-85084/HC/NHLBI NIH HHS/United States
- P30 AG024827/AG/NIA NIH HHS/United States
- R01 AG-15928/AG/NIA NIH HHS/United States
- R01 AG015928/AG/NIA NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- N01-HC-85083/HC/NHLBI NIH HHS/United States
- N01-HC-75150/HC/NHLBI NIH HHS/United States
- N01-HC-85080/HC/NHLBI NIH HHS/United States
- P50 AG005133/AG/NIA NIH HHS/United States
- P41 RR013642/RR/NCRR NIH HHS/United States
- R01 AG-20098/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
