

Real-time intra-operative near-infrared fluorescence identification of the extrahepatic bile ducts using clinically available contrast agents
- PMID: 20117813
- PMCID: PMC2886157
- DOI: 10.1016/j.surg.2009.12.004
Real-time intra-operative near-infrared fluorescence identification of the extrahepatic bile ducts using clinically available contrast agents
Abstract
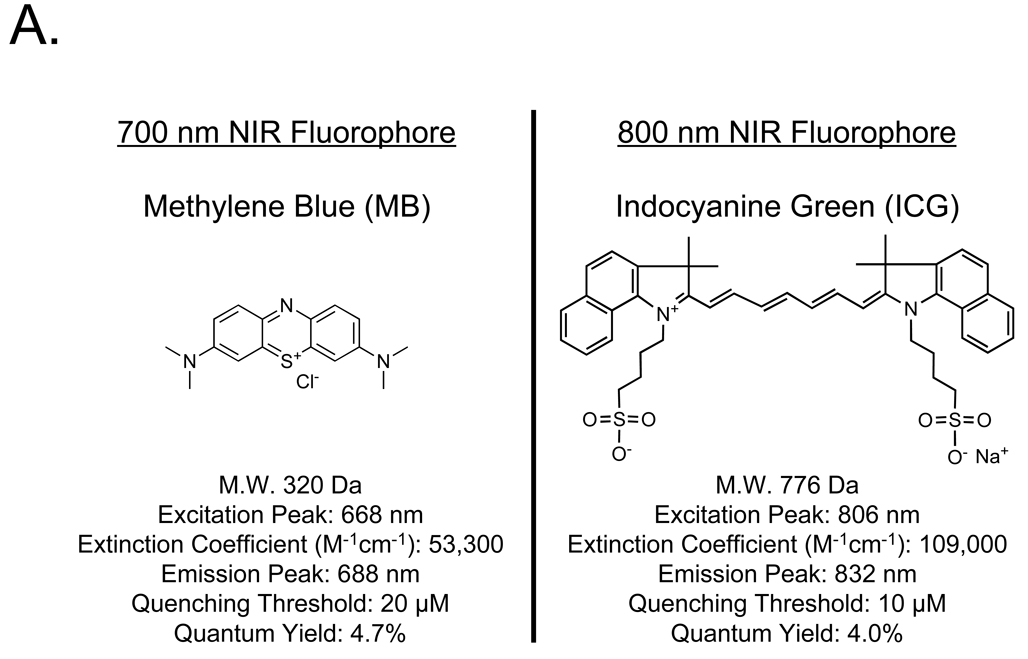
Background: Iatrogenic bile duct injuries are serious complications with patient morbidity. We hypothesized that the invisible near-infrared (NIR) fluorescence properties of methylene blue (MB) and indocyanine green (ICG) could be exploited for real-time, intraoperative imaging of the extrahepatic bile ducts during open and laparoscopic surgeries.
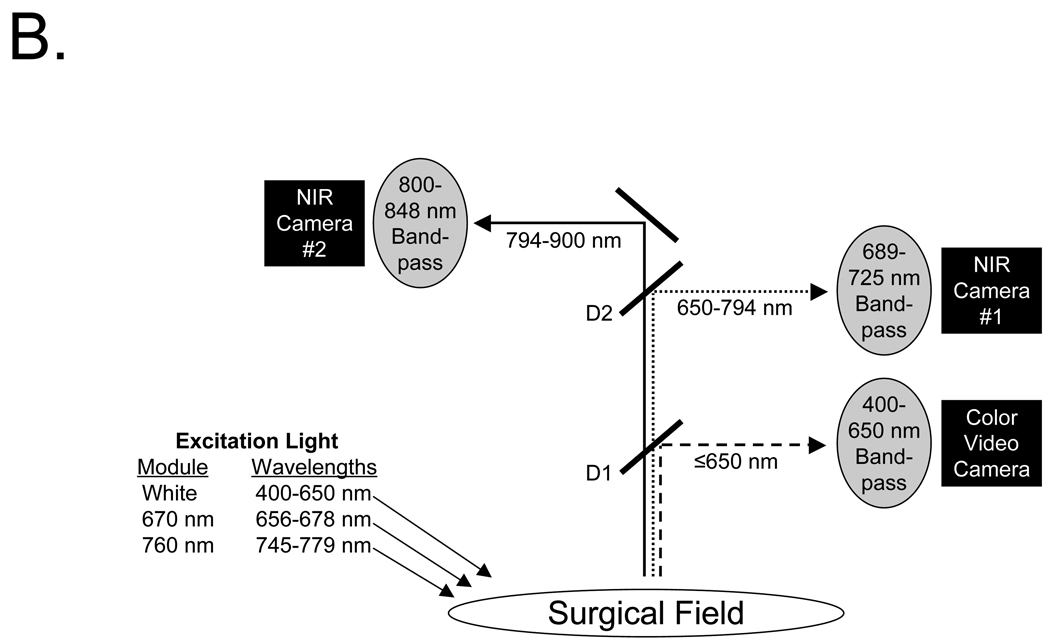
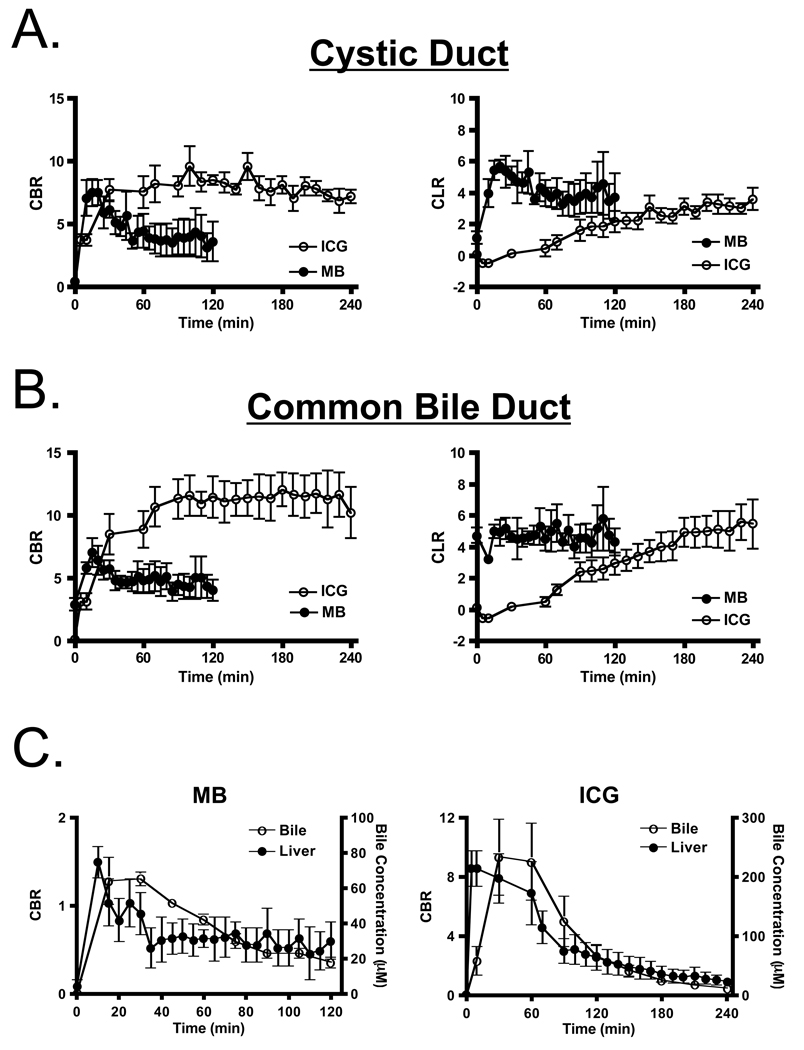
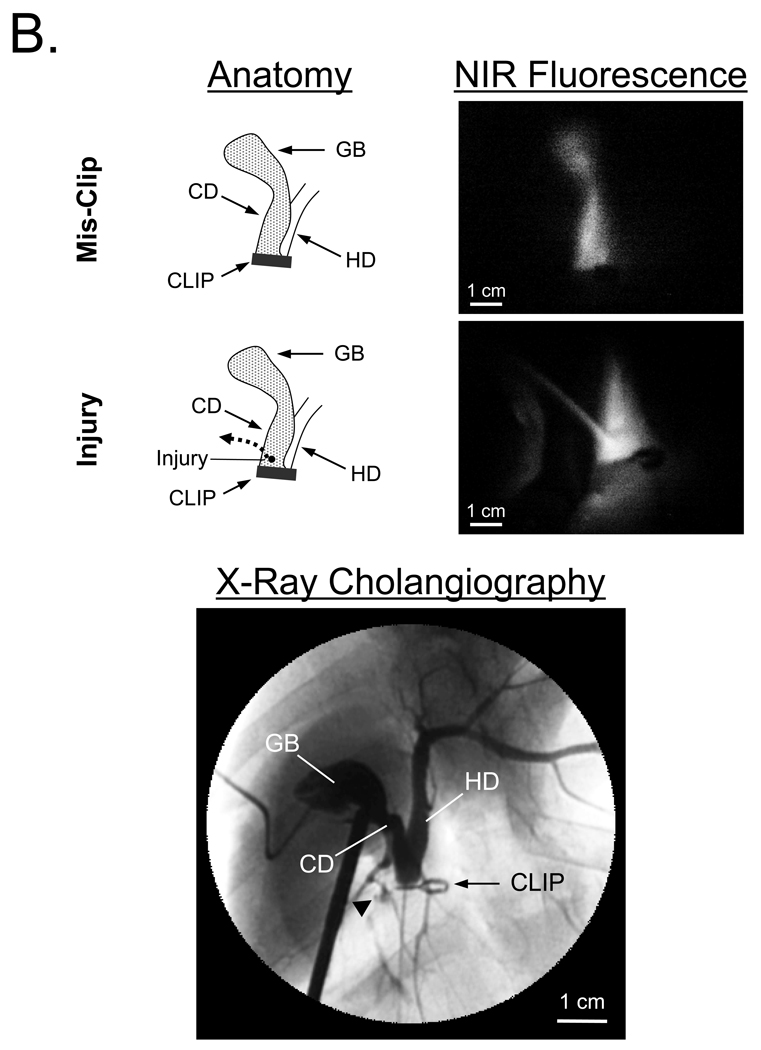
Methods: In all, 2.0 mg/kg of MB and 0.05 mg/kg of ICG were injected intravenously into 35-kg female Yorkshire pigs and the extrahepatic bile ducts were imaged over time using either the Fluorescence-Assisted Resection and Exploration (FLARE) image-guided surgery system (open surgery) or a custom NIR fluorescence laparoscopy system. Surgical anatomy was confirmed using x-ray cholangiography. The contrast-to-background ratio (CBR), contrast-to-liver ratio (CLR), and chemical concentrations in the cystic duct (CD) and common bile duct (CBD) were measured, and the performance of each agent was quantified.
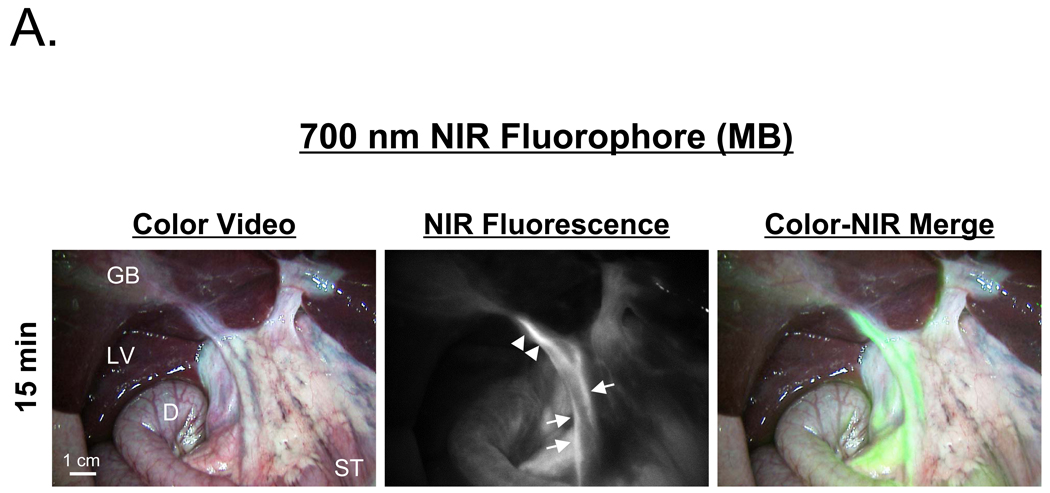
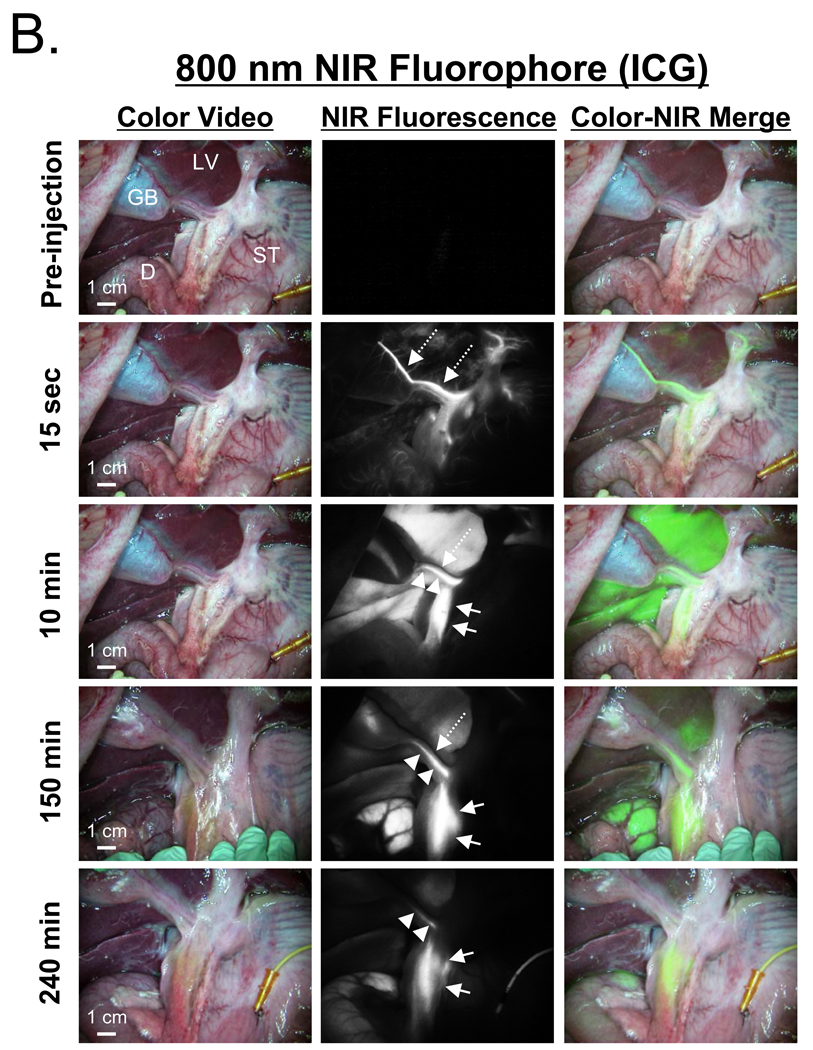
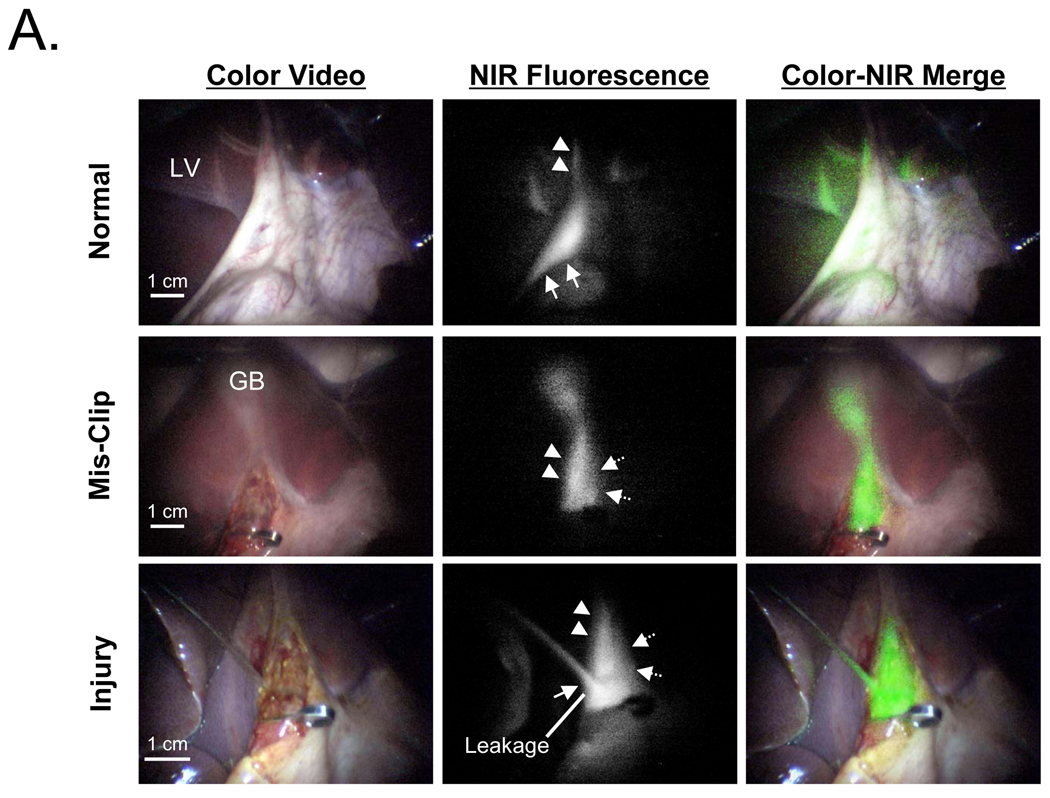
Results: Using NIR fluorescence of MB, the CD and CBD could be identified with good sensitivity (CBR and CLR > or =4), during both open and laparoscopic surgeries, from 10 to 120 min postinjection. Functional impairment of the ducts, including constriction and injury were immediately identifiable. Using NIR fluorescence of ICG, extrahepatic bile ducts did not become visible until 90 min postinjection because of strong residual liver retention; however, between 90 and 240 min, ICG provided exquisitely high sensitivity for both CD and CBD, with CBR > or =8 and CLR > or =4.
Conclusion: We demonstrate that 2 clinically available NIR fluorophores, MB fluorescing at 700 nm and ICG fluorescing at 800 nm, provide sensitive, prolonged identification of the extrahepatic bile ducts and assessment of their functional status.
Copyright 2010 Mosby, Inc. All rights reserved.
Figures
References
-
- Advance Data No. 385, Table 8. Number of all-listed procedures for discharges from short-stay hospitals by procedure category and age: United States, 2005. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics; 2007.
-
- Flum DR, Dellinger EP, Cheadle A, Chan L, Koepsell T. Intraoperative cholangiography and risk of common bile duct injury during cholecystectomy. Jama. 2003;289:1639–1644. - PubMed
-
- Nuzzo G, Giuliante F, Giovannini I, Ardito F, D'Acapito F, Vellone M, et al. Bile duct injury during laparoscopic cholecystectomy: results of an Italian national survey on 56 591 cholecystectomies. Arch Surg. 2005;140:986–992. - PubMed
-
- Savassi-Rocha PR, Almeida SR, Sanches MD, Andrade MA, Frerreira JT, Diniz MT, et al. Iatrogenic bile duct injuries. Surg Endosc. 2003;17:1356–1361. - PubMed
-
- Buanes T, Mjaland O, Waage A, Langeggen H, Holmboe J. A population-based survey of biliary surgery in Norway. Relationship between patient volume and quality of surgical treatment. Surg Endosc. 1998;12:852–855. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
