

Paclitaxel-eluting versus sirolimus-eluting stents in diabetes mellitus: a report from the National Heart, Lung, and Blood Institute Dynamic Registry
- PMID: 20118153
- PMCID: PMC2947208
- DOI: 10.1161/CIRCINTERVENTIONS.109.885996
Paclitaxel-eluting versus sirolimus-eluting stents in diabetes mellitus: a report from the National Heart, Lung, and Blood Institute Dynamic Registry
Abstract
Background: Diabetes is a powerful predictor of adverse events in patients undergoing percutaneous coronary intervention. Drug-eluting stents reduce restenosis rates compared with bare metal stents; however, controversy remains regarding which drug-eluting stents provides greater benefit in patients with diabetes. Accordingly, we compared the safety and efficacy of sirolimus-eluting stents (SES) with paclitaxel-eluting stents (PES) among diabetic patients in a contemporary registry.
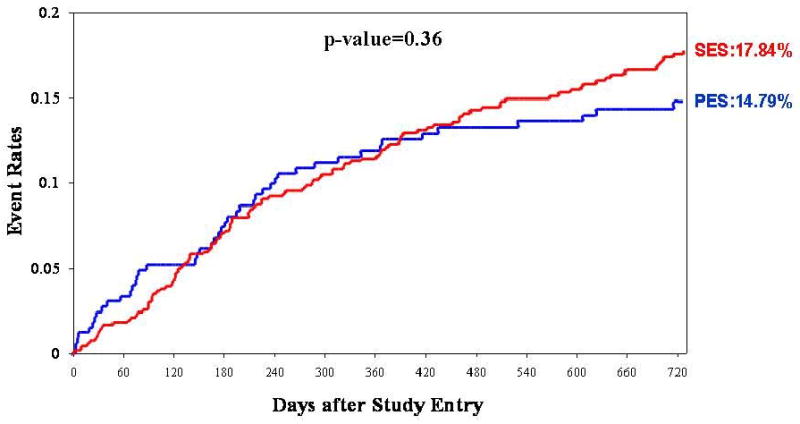
Methods and results: Using the National Heart, Lung, and Blood Institute Dynamic Registry, we evaluated 2-year outcomes of diabetic patients undergoing percutaneous coronary interventions with SES (n=677) and PES (n=328). Clinical and demographic characteristics, including age, body mass index, insulin use, left ventricular function, and aspirin/clopidogrel use postprocedure, did not differ significantly between the groups except that PES-treated patients had a greater frequency of hypertension and hyperlipidemia. At the 2-year follow-up, no significant differences were observed between PES and SES with regard to safety or efficacy end points. PES- and SES-treated patients had similar rates of death (10.7% versus 8.2%, P=0.20), death and myocardial infarction (14.9% versus 13.6%, P=0.55), repeat revascularization (14.8% versus 17.8%, P=0.36), and stent thrombosis (1.3% versus 1.3%, P=0.95). After adjustment, no significant differences between the 2 stent types in any outcome were observed.
Conclusions: PES and SES are equally efficacious and have similar safety profiles in diabetic patients undergoing percutaneous coronary interventions in clinical practice.
Figures


References
-
- Beckman JA, Creager MA, Libby P. Diabetes and atherosclerosis: epidemiology, pathophysiology, and management. JAMA. 2002;287:2570–2581. - PubMed
-
- Stein B, Weintraub WS, Gebhart SP, Cohen-Bernstein CL, Grosswald R, Liberman HA, Douglas JS, Morris DC, King SB. Influence of diabetes mellitus on early and late outcome after percutaneous transluminal coronary angioplasty. Circulation. 1995;91:979–989. - PubMed
-
- Donahoe SM, Stewart GC, McCabe CH, Mohanavelu S, Murphy SA, Cannon CP, Antman EM. Diabetes and mortality following acute coronary syndromes. JAMA. 2007;298:765–775. - PubMed
-
- Mehran R, Dangas GD, Kobayashi Y, Lansky AJ, Mintz GS, Aymong ED, Fahy M, Moses JW, Stone GW, Leon MB. Short- and long-term results after multivessel stenting in diabetic patients. J Am Coll Cardiol. 2004;43:1348–1354. - PubMed
-
- West NE, Ruygrok PN, Disco CM, Webster MW, Lindeboom WK, O'Neill WW, Mercado NF, Serruys PW. Clinical and angiographic predictors of restenosis after stent deployment in diabetic patients. Circulation. 2004;109:867–873. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
