

Transplantation of cardiac progenitor cell sheet onto infarcted heart promotes cardiogenesis and improves function
- PMID: 20118202
- PMCID: PMC2883894
- DOI: 10.1093/cvr/cvq027
Transplantation of cardiac progenitor cell sheet onto infarcted heart promotes cardiogenesis and improves function
Abstract
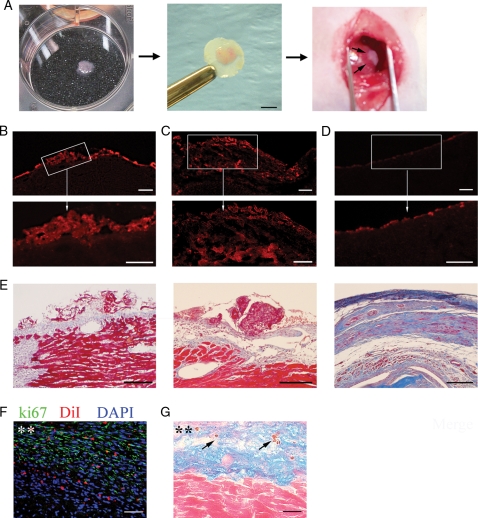
Aims: Cell-based therapy for myocardial infarction (MI) holds great promise; however, the ideal cell type and delivery system have not been established. Obstacles in the field are the massive cell death after direct injection and the small percentage of surviving cells differentiating into cardiomyocytes. To overcome these challenges we designed a novel study to deliver cardiac progenitor cells as a cell sheet.
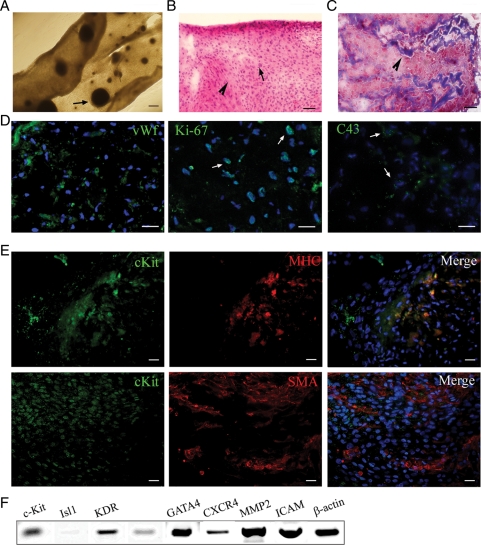
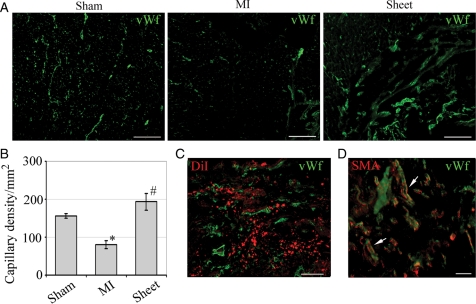
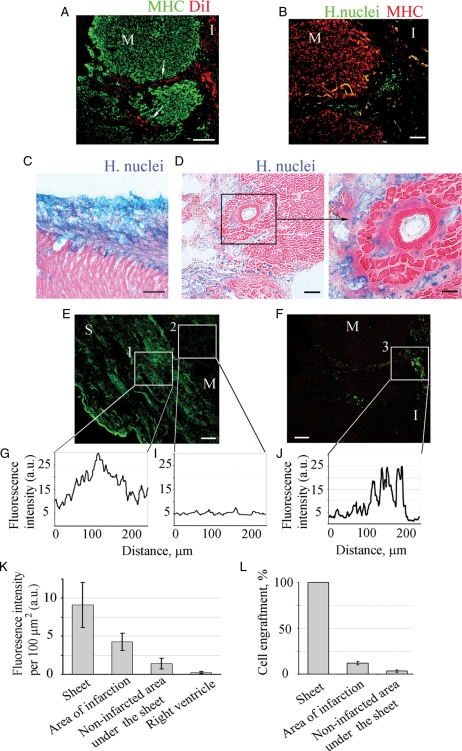
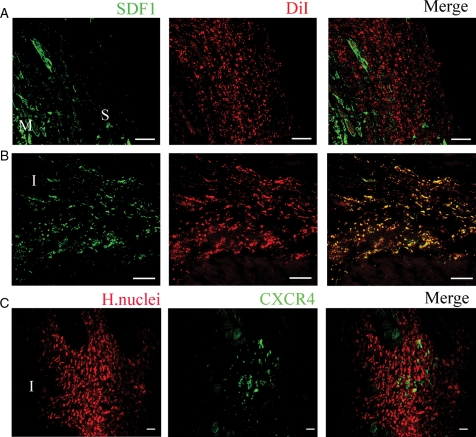
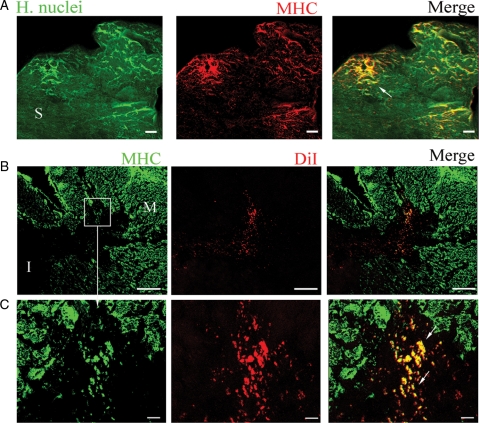
Methods and results: Cell sheets composed of rat or human cardiac progenitor cells (cardiospheres), and cardiac stromal cells were transplanted onto the infarcted myocardium after coronary artery ligation in rats. Three weeks later, transplanted cells survived, proliferated, and differentiated into cardiomyocytes (14.6 +/- 4.7%). Cell sheet transplantation suppressed cardiac wall thinning and increased capillary density (194 +/- 20 vs. 97 +/- 24 per mm(2), P < 0.05) compared with the untreated MI. Cell migration from the sheet was observed along the necrotic trails within the infarcted area. The migrated cells were located in the vicinity of stromal-derived factor (SDF-1) released from the injured myocardium, and about 20% of these cells expressed CXCR4, suggesting that the SDF-1/CXCR4 axis plays, at least, a role in cell migration. Transplantation of cell sheets resulted in a preservation of cardiac contractile function after MI, as was shown by a greater ejection fraction and lower left ventricular end diastolic pressure compared with untreated MI.
Conclusion: The scaffold-free cardiosphere-derived cell sheet approach seeks to efficiently deliver cells and increase cell survival. These transplanted cells effectively rescue myocardium function after infarction by promoting not only neovascularization but also inducing a significant level of cardiomyogenesis.
Figures
Comment in
-
Cardiac progenitor cell sheet regenerates myocardium and renews hope for translation.Cardiovasc Res. 2010 Jul 1;87(1):8-9. doi: 10.1093/cvr/cvq124. Epub 2010 Apr 29. Cardiovasc Res. 2010. PMID: 20430938 No abstract available.
References
-
- Fuchs JR, Nasseri BA, Vacanti JP, Fauza DO. Postnatal myocardial augmentation with skeletal myoblast-based fetal tissue engineering. Surgery. 2006;140:100–107. - PubMed
-
- Orlic D, Kajstura J, Chimenti S, Bodine DM, Leri A, Anversa P. Bone marrow stem cells regenerate infarcted myocardium. Pediatr Transplant. 2003;7(Suppl. 3):86–88. - PubMed
-
- Kawamoto A, Tkebuchava T, Yamaguchi J, Nishimura H, Yoon YS, Milliken C, et al. Intramyocardial transplantation of autologous endothelial progenitor cells for therapeutic neovascularization of myocardial ischemia. Circulation. 2003;107:461–468. - PubMed
-
- Iwasaki H, Kawamoto A, Ishikawa M, Oyamada A, Nakamori S, Nishimura H, et al. Dose-dependent contribution of CD34-positive cell transplantation to concurrent vasculogenesis and cardiomyogenesis for functional regenerative recovery after myocardial infarction. Circulation. 2006;113:1311–1325. - PubMed
-
- Beltrami AP, Barlucchi L, Torella D, Baker M, Limana F, Chimenti S, et al. Adult cardiac stem cells are multipotent and support myocardial regeneration. Cell. 2003;114:763–776. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
