

Clinical, etiologic, and histopathologic features of Stevens-Johnson syndrome during an 8-year period at Mayo Clinic
- PMID: 20118388
- PMCID: PMC2813820
- DOI: 10.4065/mcp.2009.0379
Clinical, etiologic, and histopathologic features of Stevens-Johnson syndrome during an 8-year period at Mayo Clinic
Abstract
Objective: To examine clinical, etiologic, and histologic features of Stevens-Johnson syndrome and to identify possible correlates of clinical disease severity related to etiologic and histopathologic findings.
Patients and methods: This is a retrospective review of patients seen at Mayo Clinic between January 1, 2000, and December 31, 2007.
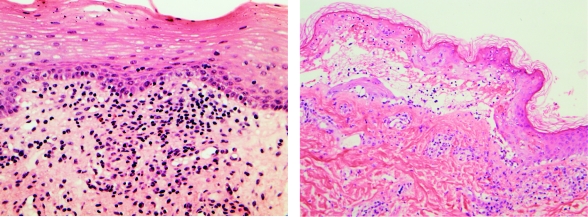
Results: Of 27 patients (mean age, 28.1 years), 22 (81%) had involvement of 2 or more mucous membranes, and 19 (70%) had ocular involvement. Medications, most commonly antibiotics and anticonvulsants, were causative in 20 patients. Mycoplasma pneumoniae infection caused 6 of the 27 cases. Corticosteroids were the most common systemic therapy. No patients with mycoplasma-induced Stevens-Johnson syndrome had internal organ involvement or required treatment in the intensive care unit, in contrast to 4 patients each in the drug-induced group. Three patients had chronic ocular sequelae, and 1 died of complications. Biopsy specimens from 13 patients (48%) showed epidermal necrosis (8 patients), basal vacuolar change (10 patients), and subepidermal bullae (10 patients). Biopsy specimens from 11 patients displayed moderate or dense dermal infiltrate. Histologic features in drug-induced cases included individual necrotic keratinocytes, dense dermal infiltrate, red blood cell extravasation, pigment incontinence, parakeratosis, and substantial eosinophils or neutrophils.
Conclusion: Our clinical and etiologic findings corroborate those in previous reports. M pneumoniae-induced Stevens-Johnson syndrome manifested less severely than its drug-induced counterpart. The limited number of biopsies precludes unequivocal demonstration of histopathologic differences between drug-induced and M pneumoniae-induced Stevens-Johnson syndrome.
Figures

References
-
- Pereira FA, Mudgil AV, Rosmarin DM. Toxic epidermal necrolysis. J Am Acad Dermatol. 2007;56(2):181-200 - PubMed
-
- Stevens AM, Johnson FC. A new eruptive fever associated with stomatitis and ophthalmia: report of two cases in children. Am J Dis Child. 1922;24:526-533
-
- Assier H, Bastuji-Garin S, Revuz J, Roujeau JC. Erythema multiforme with mucous membrane involvement and Stevens-Johnson syndrome are clinically different disorders with distinct causes. Arch Dermatol. 1995;131(5):539-543 - PubMed
-
- Bastuji-Garin S, Rzany B, Stern RS, Shear NH, Naldi L, Roujeau JC. Clinical classification of cases of toxic epidermal necrolysis, Stevens-Johnson syndrome, and erythema multiforme. Arch Dermatol. 1993;129(1):92-96 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
