

Maternal and neonatal circulating visfatin concentrations in patients with pre-eclampsia and a small-for-gestational age neonate
- PMID: 20121389
- PMCID: PMC3413321
- DOI: 10.3109/14767050903572190
Maternal and neonatal circulating visfatin concentrations in patients with pre-eclampsia and a small-for-gestational age neonate
Abstract
Objective: Maternal circulating visfatin concentrations are higher in patients with a small-for-gestational-age (SGA) neonate than in those who delivered an appropriate-for-gestational age (AGA) neonate or in those with pre-eclampsia. It has been proposed that enhanced transfer of visfatin from the foetal to maternal circulation may account for the high concentrations of maternal visfatin observed in patients with an SGA neonate. The aims of this study were: (1) to determine whether cord blood visfatin concentrations differ between normal neonates, SGA neonates and newborns of pre-eclamptic mothers; and (2) to assess the relationship between maternal and foetal circulating visfatin concentrations in patients with an SGA neonate and those with pre-eclampsia.
Study design: This cross-sectional study included 88 pregnant women and their neonates, as well as 22 preterm neonates in the following groups: (1) 44 normal pregnant women at term and their AGA neonates; (2) 22 normotensive pregnant women and their SGA neonates; (3) 22 women with pre-eclampsia and their neonates; and (4) 22 preterm neonates delivered following spontaneous preterm labour without funisitis or histologic chorioamnionitis, matched for gestational age with infants of pre-eclamptic mothers. Maternal plasma and cord blood visfatin concentrations were determined by ELISA. Non-parametric statistics were used for analyses.
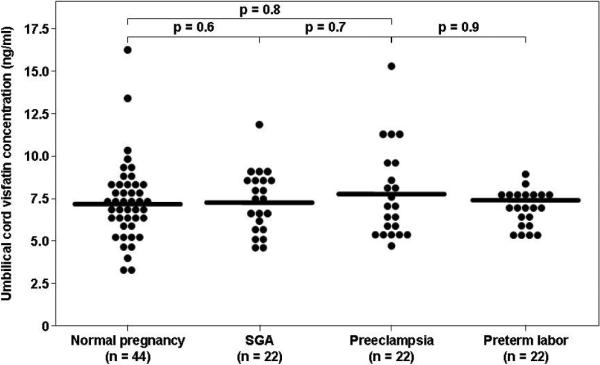
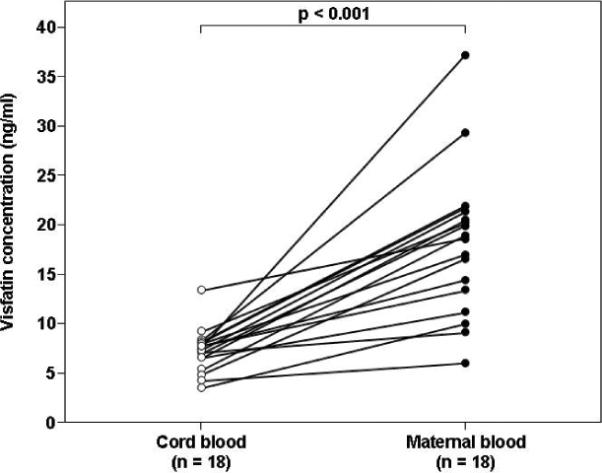
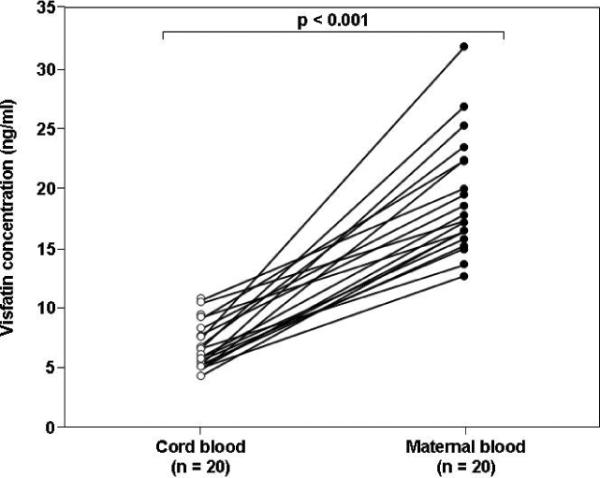
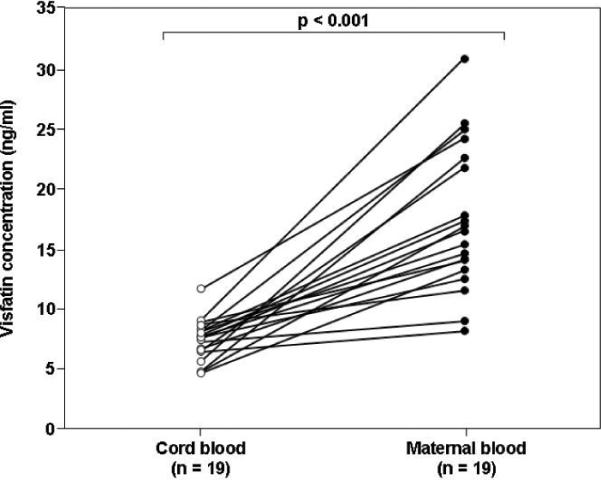
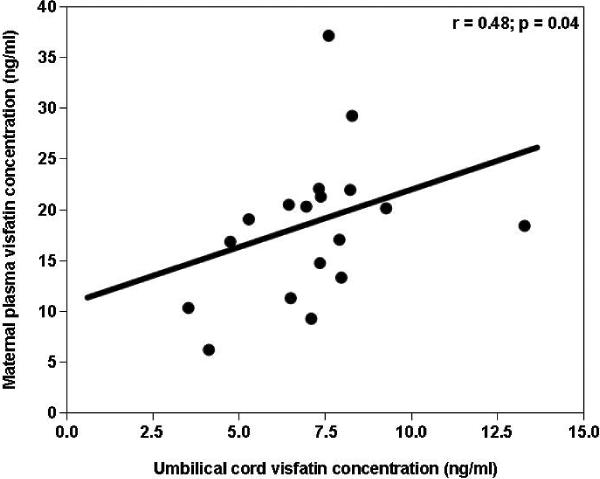
Results: (1) The median visfatin concentration was lower in umbilical cord blood than in maternal circulation, in normal pregnancy, SGA and pre-eclampsia groups (p<0.001 for all comparisons); (2) the median cord blood visfatin concentrations did not differ significantly between term AGA or SGA neonates, infants of mothers with pre-eclampsia and their gestational-age-matched preterm AGA neonates; (3) maternal and cord blood visfatin concentrations correlated only in the normal term group (r=0.48, p=0.04).
Conclusion: Circulating visfatin concentrations are lower in the foetal than in the maternal circulation and did not significantly differ between the study groups. Thus, it is unlikely that the foetal circulation is the source of the high maternal visfatin concentrations reported in patients with an SGA neonate.
Figures
Similar articles
-
Could alterations in maternal plasma visfatin concentration participate in the phenotype definition of preeclampsia and SGA?J Matern Fetal Neonatal Med. 2010 Aug;23(8):857-68. doi: 10.3109/14767050903301017. J Matern Fetal Neonatal Med. 2010. PMID: 19900033 Free PMC article.
-
Effect of intrauterine growth pattern on serum visfatin concentrations in full-term infants at birth and at 6 months of life.J Neonatal Perinatal Med. 2016;9(1):73-82. doi: 10.3233/NPM-16915029. J Neonatal Perinatal Med. 2016. PMID: 27002258
-
Evidence for differential regulation of the adipokine visfatin in the maternal and fetal compartments in normal spontaneous labor at term.J Perinat Med. 2010 May;38(3):281-8. doi: 10.1515/jpm.2010.045. J Perinat Med. 2010. PMID: 20146661 Free PMC article.
-
Visfatin in human pregnancy: maternal gestational diabetes vis-à-vis neonatal birthweight.J Perinat Med. 2009;37(3):218-31. doi: 10.1515/JPM.2009.053. J Perinat Med. 2009. PMID: 19099366 Free PMC article.
-
The role of visfatin (PBEF/Nampt) in pregnancy complications.J Reprod Immunol. 2015 Nov;112:102-10. doi: 10.1016/j.jri.2015.09.004. Epub 2015 Sep 21. J Reprod Immunol. 2015. PMID: 26451650 Review.
Cited by
-
Visfatin: New marker of oxidative stress in preterm newborns.Int J Immunopathol Pharmacol. 2016 Mar;29(1):23-9. doi: 10.1177/0394632015607952. Epub 2015 Nov 2. Int J Immunopathol Pharmacol. 2016. PMID: 26525831 Free PMC article.
-
Cord Blood Levels of Spexin, Leptin, and Visfatin in Term Infants Born Small, Appropriate, and Large for Gestational Age and Their Association with Newborn Anthropometric Measurements.J Clin Res Pediatr Endocrinol. 2022 Dec 1;14(4):444-452. doi: 10.4274/jcrpe.galenos.2022.2022-4-24. Epub 2022 Jul 21. J Clin Res Pediatr Endocrinol. 2022. PMID: 35859814 Free PMC article.
-
Characterization of Visceral and Subcutaneous Adipose Tissue Transcriptome and Biological Pathways in Pregnant and Non-Pregnant Women: Evidence for Pregnancy-Related Regional-Specific Differences in Adipose Tissue.PLoS One. 2015 Dec 4;10(12):e0143779. doi: 10.1371/journal.pone.0143779. eCollection 2015. PLoS One. 2015. PMID: 26636677 Free PMC article. Clinical Trial.
-
Placental lesions associated with maternal underperfusion are more frequent in early-onset than in late-onset preeclampsia.J Perinat Med. 2011 Nov;39(6):641-52. doi: 10.1515/jpm.2011.098. Epub 2011 Aug 17. J Perinat Med. 2011. PMID: 21848483 Free PMC article.
-
Serum adipocytokines and adiposity as predictive indices of preeclampsia.Clin Hypertens. 2020 Oct 1;26:19. doi: 10.1186/s40885-020-00152-0. eCollection 2020. Clin Hypertens. 2020. PMID: 33014422 Free PMC article.
References
-
- Di Renzo GC. The great obstetrical syndromes. J Matern Fetal Neonatal Med. 2009;22:633–635. - PubMed
-
- Gerretsen G, Huisjes HJ, Elema JD. Morphological changes of the spiral arteries in the placental bed in relation to pre-eclampsia and fetal growth retardation. Br.J.Obstet.Gynaecol. 1981;88:876–881. - PubMed
-
- Khong TY, De Wolf F, Robertson WB, Brosens I. Inadequate maternal vascular response to placentation in pregnancies complicated by pre-eclampsia and by small-for-gestational age infants. Br.J.Obstet.Gynaecol. 1986;93:1049–1059. - PubMed
-
- Chaiworapongsa T, Romero R, Espinoza J, Bujold E, Mee KY, Goncalves LF, Gomez R, Edwin S. Evidence supporting a role for blockade of the vascular endothelial growth factor system in the pathophysiology of preeclampsia. Young Investigator Award. Am.J Obstet Gynecol. 2004;190:1541–1547. - PubMed
-
- Chaiworapongsa T, Romero R, Kim YM, Kim GJ, Kim MR, Espinoza J, Bujold E, Goncalves L, Gomez R, Edwin S, et al. Plasma soluble vascular endothelial growth factor receptor-1 concentration is elevated prior to the clinical diagnosis of pre-eclampsia. J Matern.Fetal Neonatal Med. 2005;17:3–18. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous