

Predicting virologic failure in an HIV clinic
- PMID: 20121574
- PMCID: PMC3101804
- DOI: 10.1086/650537
Predicting virologic failure in an HIV clinic
Abstract
Background: We sought to use data captured in the electronic health record (EHR) to develop and validate a prediction rule for virologic failure among patients being treated for infection with human immunodeficiency virus (HIV).
Methods: We used EHRs at 2 Boston tertiary care hospitals, Massachusetts General Hospital and Brigham and Women's Hospital, to identify HIV-infected patients who were virologically suppressed (HIV RNA level < or = 400 copies/mL) on antiretroviral therapy (ART) during the period from 1 January 2005 through 31 December 2006. We used a multivariable logistic model with data from Massachusetts General Hospital to derive a 1-year virologic failure prediction rule. The model was validated using data from Brigham and Women's Hospital.We then simplified the scoring scheme to develop a clinical prediction rule.
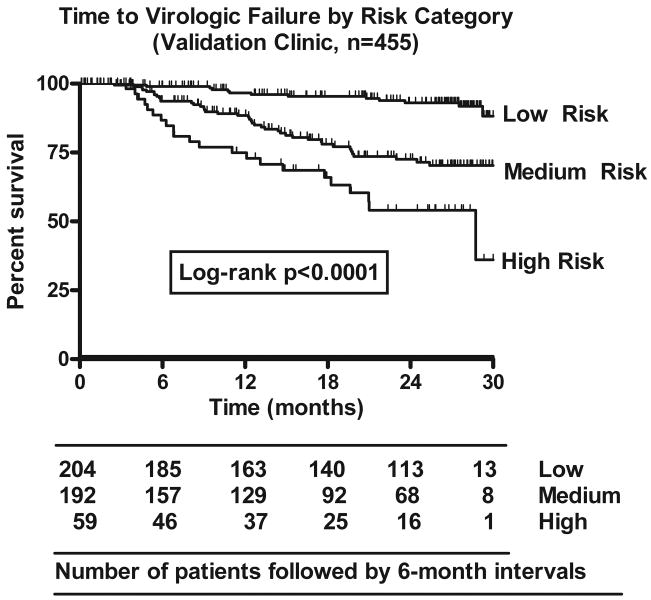
Results: The 1-year virologic failure prediction model, using data from 712 patients from Massachusetts General Hospital, demonstrated good discrimination (C statistic, 0.78) and calibration (chi(2)= 6.6; P= .58). The validation model, based on 362 patients from Brigham and Women's Hospital, also showed good discrimination (C statistic, 0.79) and calibration (chi(2)= 1.9; P= .93). The clinical prediction rule included 7 predictors (suboptimal adherence, CD4 cell count < 100 cells/microL, drug and/or alcohol abuse, highly ART experienced, missed > or = 1 appointment, prior virologic failure, and suppressed < or = 12 months) and appropriately stratified patients in the validation data set into low-, medium-, and high-risk groups, with 1-year virologic failure rates of 3.0%, 13.0%, and 28.6%, respectively.
Conclusions: A risk score based on 7 variables available in the EHR predicts HIV virologic failure at 1 year and could be used for targeted interventions to improve outcomes in HIV infection.
Conflict of interest statement
Figures


References
-
- Porter K, Babiker A, Bhaskaran K, et al. Determinants of survival following HIV-1 seroconversion after the introduction of HAART. Lancet. 2003;362:1267–74. - PubMed
-
- Palella FJ, Delaney K, Moorman A, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med. 1998;338:853–60. - PubMed
-
- Gulick RM, Ribaudo HJ, Shikuma CM, et al. Triple-nucleoside regimens versus efavirenz-containing regimens for the initial treatment of HIV-1 infection. N Engl J Med. 2004;350:1850–61. - PubMed
-
- Lucas GM, Chaisson RE, Moore RD. Highly active antiretroviral therapy in a large urban clinic: risk factors for virologic failure and adverse drug reactions. Ann Intern Med. 1999;131:81–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
