

Feline acromegaly: an essential differential diagnosis for the difficult diabetic
- PMID: 20123483
- PMCID: PMC10845472
- DOI: 10.1016/j.jfms.2009.12.003
Feline acromegaly: an essential differential diagnosis for the difficult diabetic
Abstract
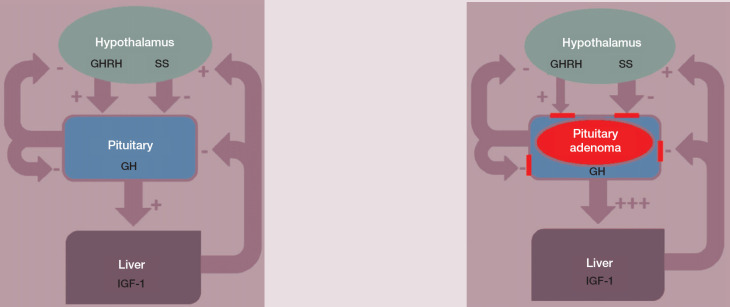
Practical relevance: Clinicians who deal with diabetic cats can have mixed experiences. Some patients are 'textbook cases', responding very well to insulin administration; others prove to be more challenging. Recent studies have shown a significant proportion of problem diabetic cats to have underlying acromegaly (hypersomatotropism). Recognising this syndrome in these cats will be key to successfully managing the concurrent diabetes.
Patient group: Just like the 'normal' (non-acromegalic) diabetic cat, the acromegalic diabetic cat tends to be a middle-aged to older male neutered domestic short hair. However, with increasing case experience, this signalment may change. Most patients are insulin resistant, although this may not be the initial presenting sign. No breed predispositions have been recognised to date.
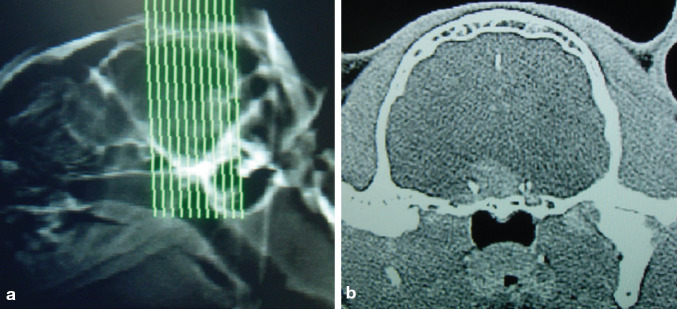
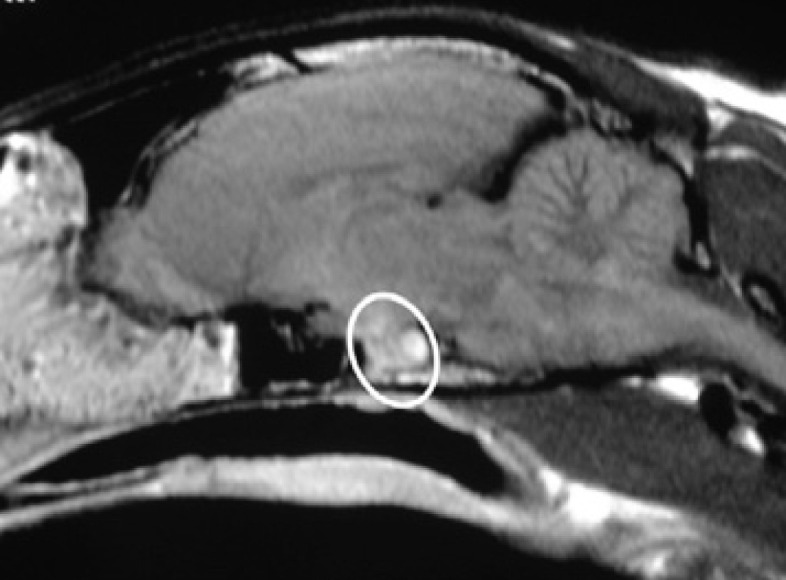
Clinical challenges: There is no single diagnostic test for feline acromegaly - a confident diagnosis relies on a combination of clinical signs, feline growth hormone and insulin-like growth factor 1 levels, and intracranial imaging. Additionally, the ideal treatment protocol has yet to be established. Currently, radiotherapy is considered by many to be the best treatment; however, costs, the need for multiple anaesthetics, and the often delayed and unpredictable treatment response represent serious limitations of this modality. Previously, medical treatment has proven unsuccessful. Recent studies provide some evidence in favour of, and some against, the use of newer long-acting somatostatin analogue preparations in a proportion of acromegalic cats.
Evidence base: Two recent studies have revealed a relatively high prevalence of acromegaly among diabetic cats. One also specifically assessed the value of hormonal tests, computed tomography and magnetic resonance imaging during the diagnostic process.
Copyright 2009 ESFM and AAFP. Published by Elsevier Ltd. All rights reserved.
Figures






References
-
- Niessen SJ, Petrie G, Gaudiano F, et al. Feline acromegaly: An underdiagnosed endocrinopathy? J Vet Intern Med 2007; 21: 899–905. - PubMed
-
- Feldman EC, Nelson RW. Disorders of growth hormone. In Feldman EC, Nelson RW. (eds). Canine and feline endocrinology and reproduction. 3rd edn. St Louis, Missouri: Saunders, 2004: p 69.
-
- Berg RI, Nelson RW, Feldman EC, et al. Serum insulin-like growth factor-I concentration in cats with diabetes mellitus and acromegaly. J Vet Intern Med 2007; 21: 892–98. - PubMed
-
- De Martino I, Visone R, Wierinckx A, et al. Fusco A proteins up-regulate CCNB2 gene in mouse and human pituitary adenomas. Cancer Res 2009; 69: 1844–50. - PubMed
-
- Niessen SJ, Khalid M, Petrie G, Church DB. Validation and application of an ovine radio-immunoassay for the diagnosis of feline acromegaly. Vet Rec 2007. 160: 902–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
