

Regional variation in carotid artery stenting and endarterectomy in the Medicare population
- PMID: 20123667
- PMCID: PMC5240818
- DOI: 10.1161/CIRCOUTCOMES.109.864736
Regional variation in carotid artery stenting and endarterectomy in the Medicare population
Abstract
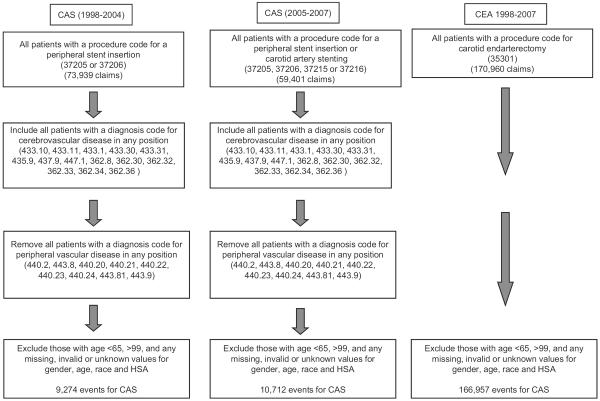
Background: To describe geographic variation in population-based rates of carotid artery stenting (CAS) and carotid endarterectomy (CEA) performed in Medicare beneficiaries.
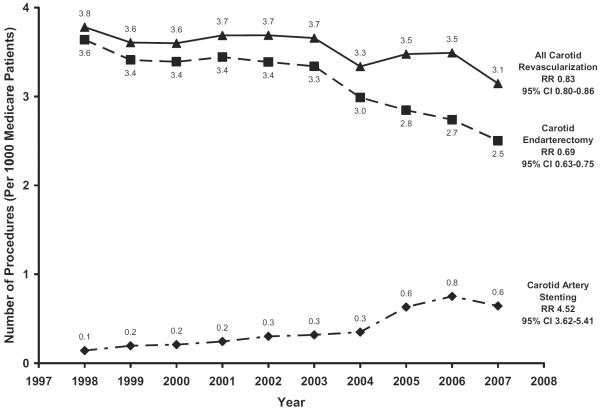
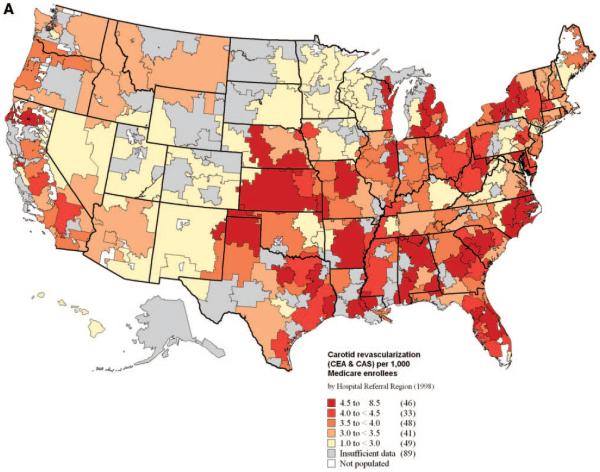
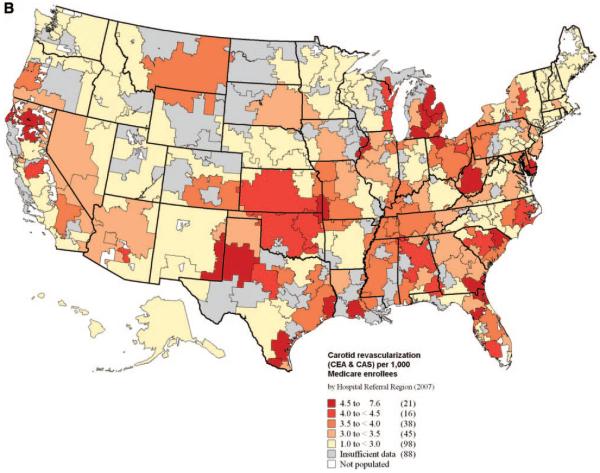
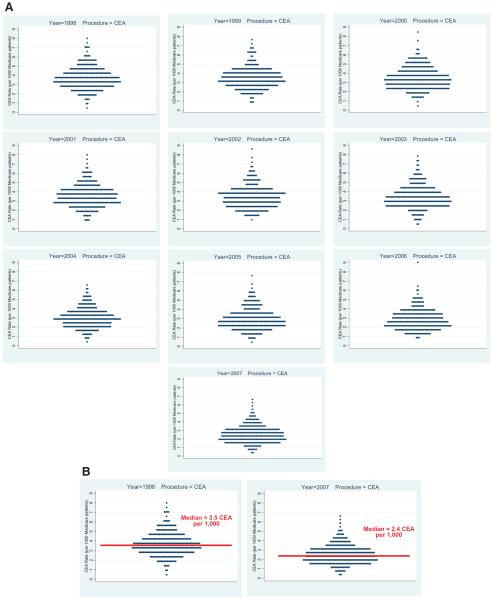
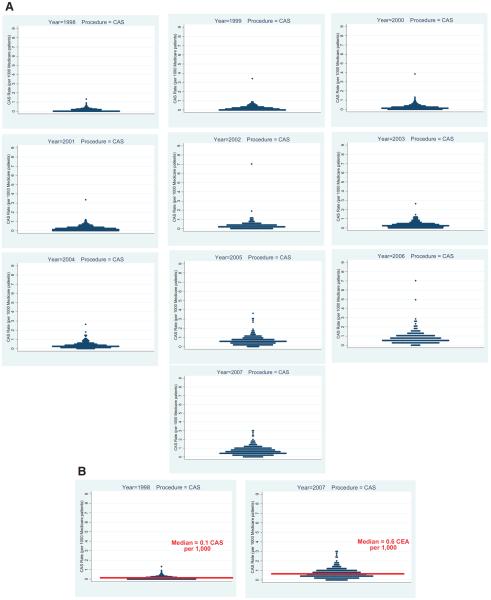
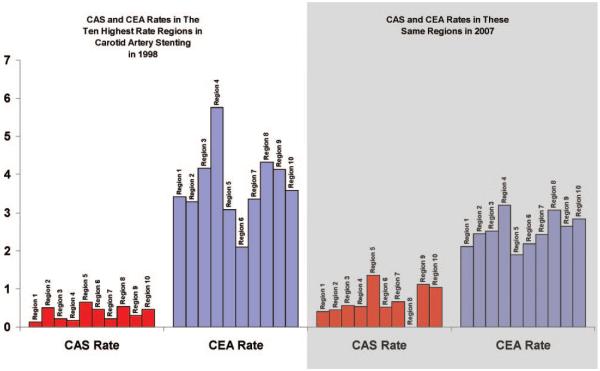
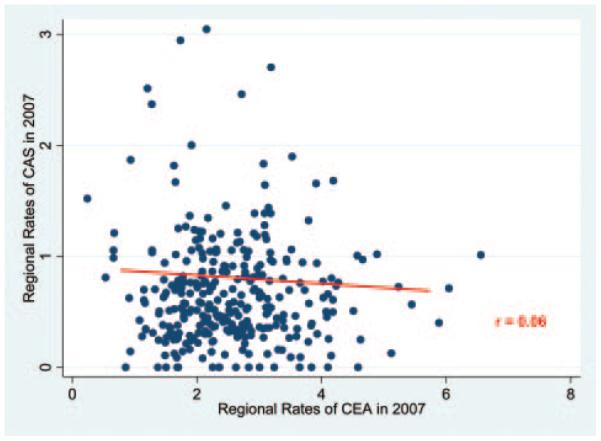
Methods and results: Medicare claims and enrollment data were used to calculate age, sex, and race-adjusted rates of CAS and CEA for Medicare beneficiaries in each of 306 hospital referral regions between 1998 and 2007. Procedures were identified using a combination of Current Procedural Terminology codes as well as diagnostic and procedural ICD-9 codes. Overall, the rate of carotid revascularization has fallen slightly over the last decade (3.8 procedures per 1000 in 1998, 3.1 procedures per 1000 in 2007; P<0.0001). Although the use of CEA decreased, from 3.6 to 2.5 procedures per 1000 beneficiaries in 2007 (P<0.0001), the use of CAS has increased >4-fold between 1998 and 2007, growing from 0.1 to 0.6 CAS procedures per 1000 beneficiaries (P<0.0001). Further, CAS rapidly disseminated across the country over the last decade. In 1998, 66% of hospital referral regions had a hospital that performed CAS; however, by 2007, nearly all (95%) hospital referral regions performed CAS (P<0.0001). Last, in regions with the highest utilization rates of CAS, it appeared that CAS was performed as a substitute for CEA. There was little evidence that CAS was being performed in addition to CEA, as no correlation existed between regional rates of CAS and CEA (r=0.06).
Conclusions: Even though CEA was used less frequently in 2007 than 1998, the use of CAS has grown significantly. Although regional variation in the use of CEA has remained fairly constant, regional variation has increased in the use of CAS. Given these changes in practice patterns, careful examination of the efficacy and cost-effectiveness of CAS is necessary.
Figures
Comment in
-
Regional variation: only moderately interesting: a word of caution.Circ Cardiovasc Qual Outcomes. 2010 Jan;3(1):6-7. doi: 10.1161/CIRCOUTCOMES.109.927103. Circ Cardiovasc Qual Outcomes. 2010. PMID: 20123665 No abstract available.
References
-
- Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. Endarterectomy for asymptomatic carotid artery stenosis. JAMA. 1995;273:1421–1428. - PubMed
-
- Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis: North American Symptomatic Carotid End-arterectomy Trial Collaborators. N Engl J Med. 1991;325:445–453. - PubMed
-
- Goodney PP, Schermerhorn ML, Powell RJ. Current status of carotid artery stenting. J Vasc Surg. 2006;43:406–411. - PubMed
-
- Wholey MH, Al-Mubarek N. Updated review of the global carotid artery stent registry. Catheter Cardiovasc Intervent. 2003;60:259–266. - PubMed
-
- Goullard L, Gommeaux A, Poncelet P, Lenica D, Durand P, Dieux C. [Asymptomatic carotid stenoses: a cardiologist's viewpoint.] Ann Cardiol Angeiol. 2004;53:54–59. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
