

Determinants of cardiac catheterization use in older Medicare patients with acute myocardial infarction
- PMID: 20123672
- PMCID: PMC3024143
- DOI: 10.1161/CIRCOUTCOMES.109.858456
Determinants of cardiac catheterization use in older Medicare patients with acute myocardial infarction
Abstract
Background: Cardiac catheterization is substantially underused among higher-risk patients with acute myocardial infarction (AMI) with appropriate indications but overused among patients with inappropriate indications. We sought to determine the importance of anticipated benefit and anticipated harm on the use of cardiac catheterization among older patients with AMI.
Methods and results: We performed an analysis of Medicare fee-for-service beneficiaries hospitalized with an AMI between 1998 and 2001. Multivariate models were developed to determine relative importance of anticipated benefit (baseline cardiovascular risk), anticipated harm (bleeding risk, comorbidities), and demographic factors (age, sex, race, regional invasive intensity) in predicting cardiac catheterization use within 60 days of AMI admission. Analyses were stratified by American College of Cardiology/American Heart Association class I or II as appropriate, and class III as inappropriate. Determinants of reduced likelihood of cardiac catheterization among 42 241 AMI patients with appropriate indications included (in order of importance) older age (likelihood chi(2)=1309.5), higher bleeding risk score (likelihood chi(2)=471.2), more comorbidities (likelihood chi(2)=276.6), female sex (likelihood chi(2)=162.9), hospitalization in low (likelihood chi(2)=67.9) or intermediate intensity invasive regions (likelihood chi(2)=22.4) (all P<0.001), and baseline cardiovascular risk (likelihood chi(2)=6.4, P=0.01). Among 2398 AMI patients with inappropriate indications, significant determinants of greater procedure likelihood included younger age, male sex, lower bleeding risk score, and fewer comorbidities.
Conclusions: Regardless of the procedure indication, the decision to perform cardiac catheterization in this population appears largely driven by demographic factors and potential harm rather than potential benefit of the procedure.
Figures
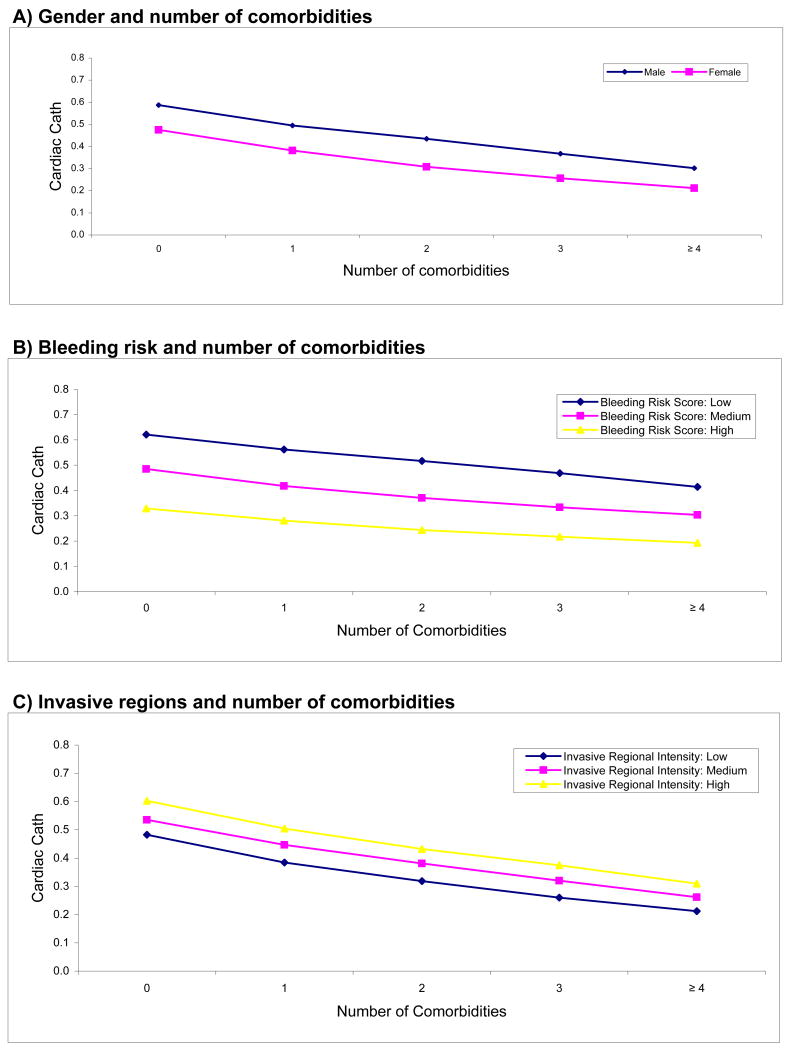
Figure 1a) Gender and number of comorbidities
Figure 1b) Bleeding risk and number of comorbidities
Figure 1c) Invasive regional intensity and number of comorbidities
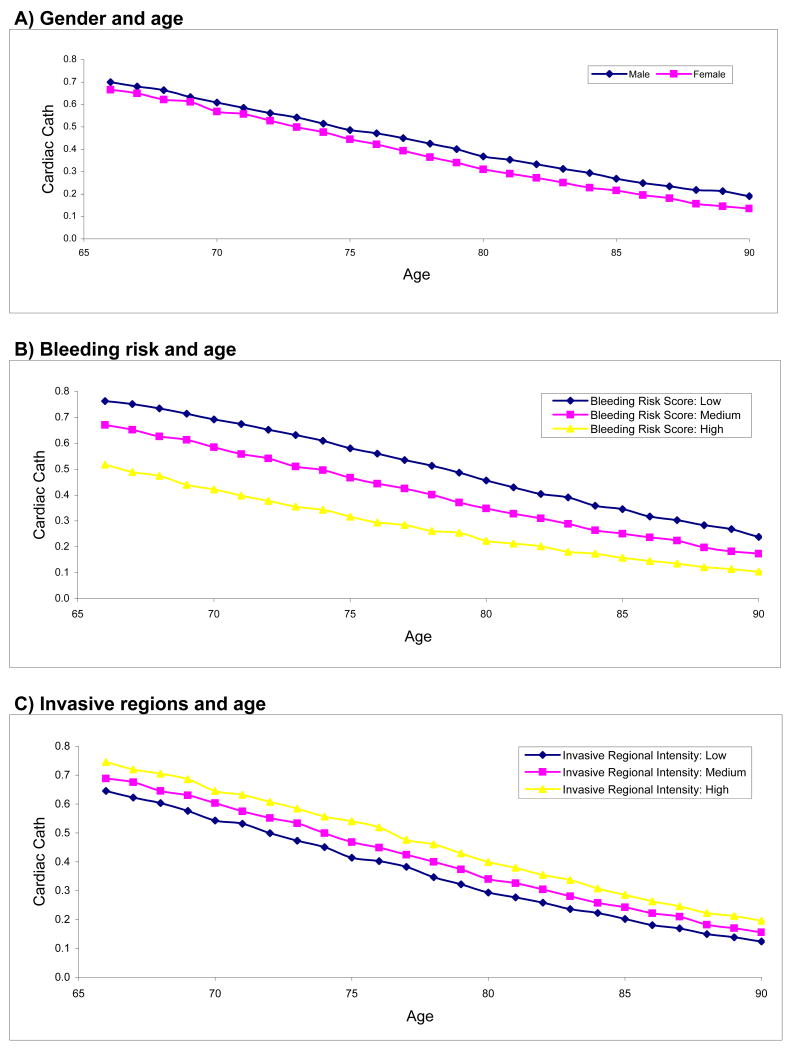
Figure 2a) Gender and age
Figure 2b) Bleeding risk and age
Figure 2c) Invasive regional intensity and age
Similar articles
-
Regional variation in cardiac catheterization appropriateness and baseline risk after acute myocardial infarction.J Am Coll Cardiol. 2008 Feb 19;51(7):716-23. doi: 10.1016/j.jacc.2007.10.039. J Am Coll Cardiol. 2008. PMID: 18279735
-
Sex differences in cardiac catheterization: the role of physician gender.JAMA. 2001 Dec 12;286(22):2849-56. doi: 10.1001/jama.286.22.2849. JAMA. 2001. PMID: 11735761
-
Racial differences in the use of cardiac catheterization after acute myocardial infarction.N Engl J Med. 2001 May 10;344(19):1443-9. doi: 10.1056/NEJM200105103441906. N Engl J Med. 2001. PMID: 11346810
-
Race and sex differences in the refusal of cardiac catheterization among elderly patients hospitalized with acute myocardial infarction.Am Heart J. 2002 Dec;144(6):1052-6. doi: 10.1067/mhj.2002.126122. Am Heart J. 2002. PMID: 12486430
-
Upper endoscopy in patients with acute myocardial infarction and upper gastrointestinal bleeding: results of a decision analysis.Dig Dis Sci. 2009 Apr;54(4):701-11. doi: 10.1007/s10620-008-0403-y. Epub 2008 Jul 26. Dig Dis Sci. 2009. PMID: 18661236 Free PMC article. Review.
Cited by
-
Race/Ethnicity and overuse of care: a systematic review.Milbank Q. 2015 Mar;93(1):112-38. doi: 10.1111/1468-0009.12107. Milbank Q. 2015. PMID: 25752352 Free PMC article.
-
Determinants of invasive strategy in elderly patients with non-ST elevation myocardial infarction.J Geriatr Cardiol. 2017 Jul;14(7):465-472. doi: 10.11909/j.issn.1671-5411.2017.07.001. J Geriatr Cardiol. 2017. PMID: 28868075 Free PMC article.
-
Acute coronary syndromes in octogenarians referred for invasive evaluation: treatment profile and outcomes.Clin Res Cardiol. 2015 Jan;104(1):51-8. doi: 10.1007/s00392-014-0756-5. Epub 2014 Aug 21. Clin Res Cardiol. 2015. PMID: 25142902
-
External adjustment sensitivity analysis for unmeasured confounding: an application to coronary stent outcomes, Pennsylvania 2004-2008.Health Serv Res. 2013 Jun;48(3):1191-214. doi: 10.1111/1475-6773.12013. Epub 2012 Dec 3. Health Serv Res. 2013. PMID: 23206261 Free PMC article.
-
Regional density of cardiologists and rates of mortality for acute myocardial infarction and heart failure.Circ Cardiovasc Qual Outcomes. 2013 May 1;6(3):352-9. doi: 10.1161/CIRCOUTCOMES.113.000214. Epub 2013 May 16. Circ Cardiovasc Qual Outcomes. 2013. PMID: 23680965 Free PMC article.
References
-
- Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE, Jr, Chavey WE, 2nd, Fesmire FM, Hochman JS, Levin TN, Lincoff AM, Peterson ED, Theroux P, Wenger NK, Wright RS, Smith SC, Jr, Jacobs AK, Halperin JL, Hunt SA, Krumholz HM, Kushner FG, Lytle BW, Nishimura R, Ornato JP, Page RL, Riegel B. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non ST-Elevation Myocardial Infarction): developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons: endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. Circulation. 2007;116:e148–304. - PubMed
-
- Antman EM, Hand M, Armstrong PW, Bates ER, Green LA, Halasyamani LK, Hochman JS, Krumholz HM, Lamas GA, Mullany CJ, Pearle DL, Sloan MA, Smith SC, Jr, Anbe DT, Kushner FG, Ornato JP, Jacobs AK, Adams CD, Anderson JL, Buller CE, Creager MA, Ettinger SM, Halperin JL, Hunt SA, Lytle BW, Nishimura R, Page RL, Riegel B, Tarkington LG, Yancy CW. 2007 focused update of the ACC/AHA 2004 guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the Canadian Cardiovascular Society endorsed by the American Academy of Family Physicians: 2007 Writing Group to Review New Evidence and Update the ACC/AHA 2004 Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction, Writing on Behalf of the 2004 Writing Committee. Circulation. 2008;117:296–329. - PubMed
-
- Bhatt DL, Roe MT, Peterson ED, Li Y, Chen AY, Harrington RA, Greenbaum AB, Berger PB, Cannon CP, Cohen DJ, Gibson CM, Saucedo JF, Kleiman NS, Hochman JS, Boden WE, Brindis RG, Peacock WF, Smith SC, Jr, Pollack CV, Jr, Gibler WB, Ohman EM. for the CRUSADE Investigators. Utilization of early invasive management strategies for high-risk patients with non-ST-segment elevation acute coronary syndromes: results from the CRUSADE Quality Improvement Initiative. JAMA. 2004;292:2096–2104. - PubMed
-
- Fox KA, Anderson FA, Dabbous OH, Steg PG, Lopez-Sendon JL, Van de Werf F, Budaj A, Gurfinkel EP, Goodman SG, Brieger D. Intervention in acute coronary syndromes: do patients undergo intervention on the basis of their risk characteristics? The Global Registry of Acute Coronary Events (GRACE) Heart. 2007;93:177–182. - PMC - PubMed
-
- Ko DT, Krumholz HM, Wang Y, Foody JM, Masoudi FA, Havranek EP, You JJ, Alter DA, Stukel TA, Newman AM, Tu JV. Regional differences in process of care and outcomes for older acute myocardial infarction patients in the United States and Ontario, Canada. Circulation. 2007;115:196–203. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
