

Socio-economic and ethnic group inequities in antenatal care quality in the public and private sector in Brazil
- PMID: 20123940
- PMCID: PMC2889278
- DOI: 10.1093/heapol/czp065
Socio-economic and ethnic group inequities in antenatal care quality in the public and private sector in Brazil
Abstract
Background: Socio-economic inequalities in maternal and child health are ubiquitous, but limited information is available on how much the quality of care varies according to wealth or ethnicity in low- and middle-income countries. Also, little information exists on quality differences between public and private providers.
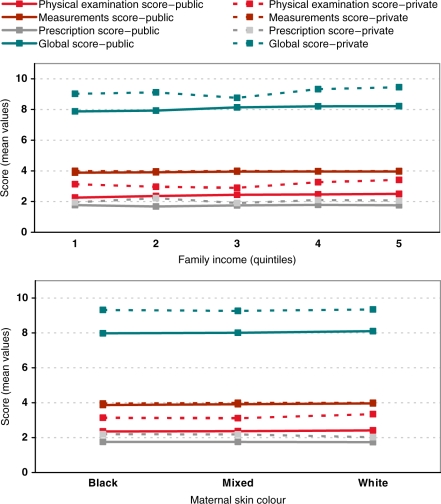
Methods: Quality of care for women giving birth in 2004 in Pelotas, Brazil, was assessed by measuring how many of 11 procedures recommended by the Ministry of Health were performed. Information on family income, self-assessed skin colour, parity and type of provider were collected.
Results: Antenatal care was used by 98% of the 4244 women studied (mean number of visits 8.3), but the number of consultations was higher among better-off and white women, who were also more likely to start antenatal care in the first trimester. The quality of antenatal care score ranged from 0 to 11, with an overall mean of 8.3 (SD 1.7). Mean scores were 8.9 (SD 1.5) in the wealthiest and 7.9 (SD 1.8) in the poorest quintiles (P < 0.001), 8.4 (SD 1.6) in white and 8.1 (SD 1.9) in black women (P < 0.001). Adjusted analyses showed that these differences seemed to be due to attendance patterns rather than discrimination. Mean quality scores were higher in the private 9.3 (SD 1.3) than in the public sector 8.1 (SD 1.6) (P < 0.001); these differences were not explained by maternal characteristics or by attendance patterns.
Conclusions: Special efforts must be made to improve quality of care in the public sector. Poor and black women should be actively encouraged to start antenatal care early in pregnancy so that they can fully benefit from it. There is a need for regular monitoring of antenatal attendances and quality of care with an equity lens, in order to assess how different social groups are benefiting from progress in health care.
Figures
References
-
- ACOG–Committee on Health Care for Underserved Women. ACOG committee opinion. Number 317, October 2005. Racial and ethnic disparities in women’s health. Obstetrics & Gynecology. 2005;106:889–92. - PubMed
-
- Almeida SD, Barros MB. Equity and access to health care for pregnant women in Campinas (SP), Brazil. Revista Panamericana de Salud Publica. 2005;17:15–25. - PubMed
-
- Bailie RS, Selvey CE, Bourne D, et al. Trends in cervical cancer mortality in South Africa. International Journal of Epidemiology. 1996;25:488–93. - PubMed
-
- Barros AJ, Bertoldi AD. Out-of-pocket health expenditure in a population covered by the Family Health Program in Brazil. International Journal of Epidemiology. 2008;37:758–65. - PubMed
-
- Barros FC, Victora CG. Iniqüidades em saúde de crianças menores de cinco anos no Brasil. Uma revisão sistemática da literatura, 1990–2007. Rio de Janeiro: 2007.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
