

Time trends and local variation in primary treatment of localized prostate cancer
- PMID: 20124165
- PMCID: PMC2834465
- DOI: 10.1200/JCO.2009.26.0133
Time trends and local variation in primary treatment of localized prostate cancer
Abstract
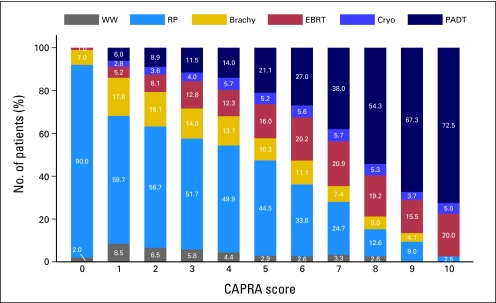
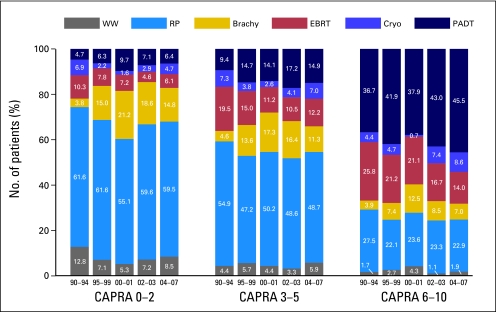
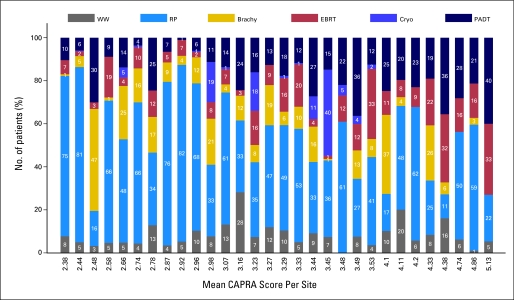
PURPOSE In the absence of high-level evidence or clinical guidelines supporting any given active treatment approach over another for localized prostate cancer, clinician and patient preferences may lead to substantial variation in treatment use. METHODS Data were analyzed from 36 clinical sites that contributed data to the Cancer of the Prostate Strategic Urologic Research Endeavor (CaPSURE) registry. Distribution of primary treatment use was measured over time. Prostate cancer risk was assessed using the D'Amico risk groups and the Cancer of the Prostate Risk Assessment (CAPRA) score. Descriptive analyses were performed, and a hierarchical model was constructed that controlled for year of diagnosis, cancer risk variables, and other patient factors to estimate the proportion of variation in primary treatment selection explicable by practice site. Results Among 11,892 men analyzed, 6.8% elected surveillance, 49.9% prostatectomy, 11.6% external-beam radiation, 13.3% brachytherapy, 4.0% cryoablation, and 14.4% androgen deprivation monotherapy. Prostate cancer risk drives treatment selection, but the data suggest both overtreatment of low-risk disease and undertreatment of high-risk disease. The former trend appears to be improving over time, while the latter is worsening. Treatment varies with age, comorbidity, and socioeconomic status. However, treatment patterns vary markedly across clinical sites, and this variation is not explained by case-mix variability or known patient factors. Practice site explains a proportion of this variation ranging from 13% for androgen deprivation monotherapy to 74% for cryoablation. CONCLUSION Substantial variation exists in management of localized prostate cancer that is not explained by measurable factors. A critical need exists for high-quality comparative effectiveness research in localized prostate cancer to help guide treatment decision making.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Outcomes for radical prostatectomy: is it the singer, the song, or both?J Clin Oncol. 2012 Feb 10;30(5):476-8. doi: 10.1200/JCO.2011.38.9593. Epub 2012 Jan 3. J Clin Oncol. 2012. PMID: 22215744 No abstract available.
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2009. CA Cancer J Clin. 2009;59:225–249. - PubMed
-
- Wei JT, Dunn RL, Sandler HM, et al. Comprehensive comparison of health-related quality of life after contemporary therapies for localized prostate cancer. J Clin Oncol. 2002;20:557–566. - PubMed
-
- Wilt TJ, MacDonald R, Rutks I, et al. Systematic review: Comparative effectiveness and harms of treatments for clinically localized prostate cancer. Ann Intern Med. 2008;148:435–448. - PubMed
-
- Thompson I, Thrasher JB, Aus G, et al. Guideline for the management of clinically localized prostate cancer: 2007 update. J Urol. 2007;177:2106–2131. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
