

Finasteride to prevent prostate cancer: should all men or only a high-risk subgroup be treated?
- PMID: 20124185
- PMCID: PMC2834464
- DOI: 10.1200/JCO.2009.23.5572
Finasteride to prevent prostate cancer: should all men or only a high-risk subgroup be treated?
Abstract
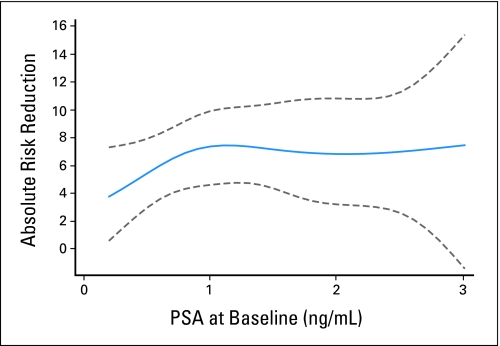
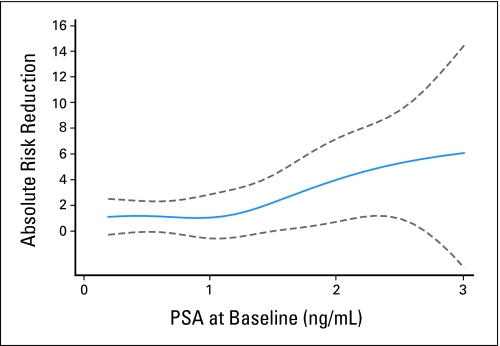
PURPOSE Finasteride has been shown to reduce the incidence of prostate cancer. Yet the use of finasteride remains low, likely because of the risk of adverse effects. We sought to determine whether prostate-specific antigen (PSA) levels could identify a high-risk subgroup for which the benefits of finasteride treatment outweigh the potential harms. PATIENTS AND METHODS Raw data from the Prostate Cancer Prevention Trial were used to model chemopreventive treatment strategies: treat all men, treat no men, or treat a high-risk subgroup based on PSA level. We weighted the benefits (reduction in cancer rate) and harms (treatment rate) of each strategy using numbers-needed-to-treat thresholds-the maximum number of men a clinician would treat with finasteride to prevent one cancer. Results Of 9,058 men, 1,957 were diagnosed with prostate cancer during the 7-year study. For the end point of all cancers, including both for-cause and end-of-study biopsies, the optimal strategy is to treat all or nearly all men. To reduce risk of cancers detected through routine care, treating men with PSA > 1.3 or > 2 ng/mL is optimal. For example, treating only men with PSA > 2 ng/mL reduced the treatment rate by 83% and resulted in a cancer rate only 1.1% higher than treating all men. CONCLUSION Clinicians wishing to reduce the risk of any biopsy-detectable prostate cancer should recommend finasteride to all men. Clinicians who believe that it is unnecessary to prevent all cancers, but that preventing those readily detectable by screening would be desirable, would be best off recommending finasteride only to a high-risk subgroup.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Optimizing finasteride chemoprevention.Nat Rev Urol. 2010 Apr;7(4):178. doi: 10.1038/nrurol.2010.33. Nat Rev Urol. 2010. PMID: 20397282 No abstract available.
-
Chemotherapy: Optimizing finasteride chemoprevention for prostate cancer.Nat Rev Clin Oncol. 2010 May;7(5):242. doi: 10.1038/nrclinonc.2010.53. Nat Rev Clin Oncol. 2010. PMID: 20432528 No abstract available.
References
-
- Thompson IM, Goodman PJ, Tangen CM, et al. The influence of finasteride on the development of prostate cancer. N Engl J Med. 2003;349:215–224. - PubMed
-
- Goetzl MA, Holzbeierlein JM. Finasteride as a chemopreventive agent in prostate cancer: Impact of the PCPT on urologic practice. Nat Clin Pract Urol. 2006;3:422–429. - PubMed
-
- Kulkarni GS, Al-Azab R, Lockwood G, et al. Evidence for a biopsy derived grade artifact among larger prostate glands. J Urol. 2006;175:505–509. - PubMed
-
- Lucia MS, Epstein JI, Goodman PJ, et al. Finasteride and high-grade prostate cancer in the Prostate Cancer Prevention Trial. J Natl Cancer Inst. 2007;99:1375–1383. - PubMed
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2009. CA Cancer J Clin. 2009;59:225–49. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
