

Gastroscopically controlled laparoscopic sleeve gastrectomy
- PMID: 20124771
- PMCID: PMC6444463
- DOI: 10.1159/000198242
Gastroscopically controlled laparoscopic sleeve gastrectomy
Abstract
Background: Laparoscopic sleeve gastrectomy is becoming increasingly established as a stand-alone procedure for weight reduction. The restrictive as well as humoral characteristics of this operation assure postoperative weight loss of up to 70-80% after 1 year. Complications also occur with this procedure.
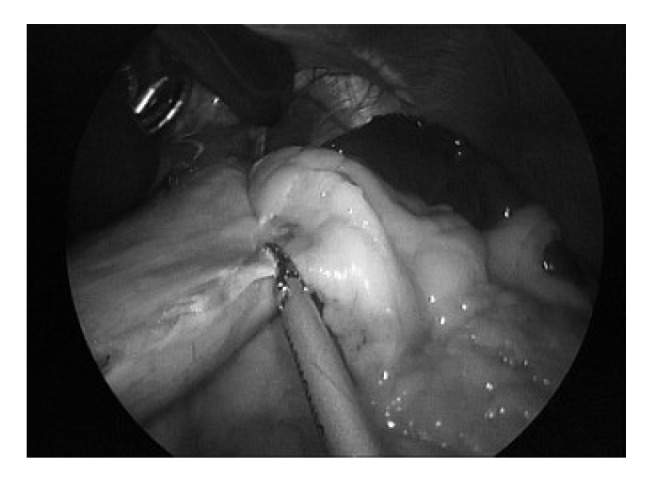
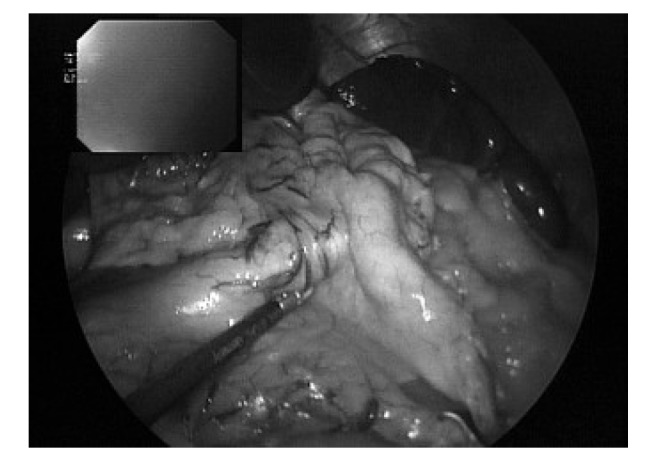
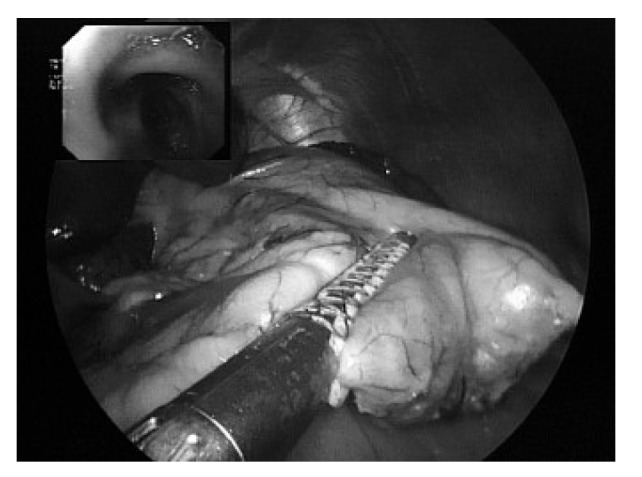
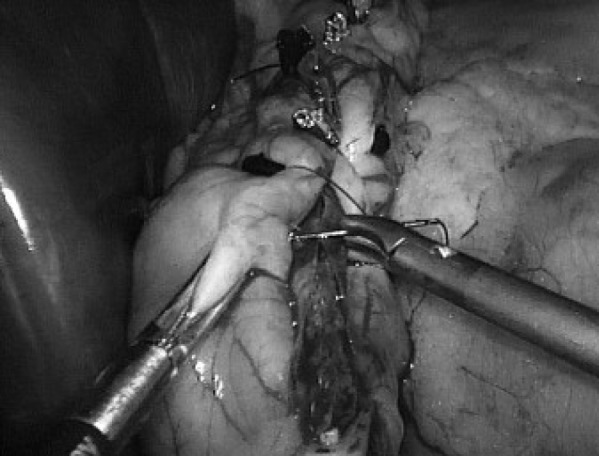
Methods: The technical details of the sleeve gastrectomy surgical procedure are described, while elaborating on potential complications and on calibration. In our case, we perform gastrectomy under intraoperative gastroscopic control for calibration as well as for suture control as a standard procedure. As a general practice, the staple line is reinforced with the bioabsorbable material Seamguard.
Results: Since June 2006, 38 patients have undergone sleeve gastrectomy.Postsurgical bleeding occurred in 1 case (2.6%) and had to be treated surgically. 1 patient developed cicatricial stenosis and required dilatation (2.6%). After 1 year, 85% of patients had a weight loss of 70-80%.
Conclusion: Thanks to the standardisation of this procedure using staple line reinforcement and intraoperative gastroscopic control, the complication rate can be reduced and the successful outcome of this stand-alone,weight-reduction operation can be optimised.
Figures
Similar articles
-
Is There Necessity for Oversewing the Staple Line During Laparoscopic Sleeve Gastrectomy? An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials.J Invest Surg. 2020 Oct;33(9):839-850. doi: 10.1080/08941939.2019.1665380. Epub 2019 Dec 5. J Invest Surg. 2020. PMID: 31805796
-
Staple line reinforcement during sleeve gastrectomy with a new type of reinforced stapler.Minerva Chir. 2018 Apr;73(2):127-132. doi: 10.23736/S0026-4733.18.07627-7. Epub 2018 Feb 1. Minerva Chir. 2018. PMID: 29397639
-
Bioabsorbable Glycolide Copolymer is Effective in Reducing Staple Line Bleeding in Sleeve Gastrectomy.Obes Surg. 2022 Aug;32(8):2605-2610. doi: 10.1007/s11695-022-06152-3. Epub 2022 Jun 13. Obes Surg. 2022. PMID: 35696051
-
Sleeve Gastrectomy: Surgical Tips.J Laparoendosc Adv Surg Tech A. 2018 Aug;28(8):930-937. doi: 10.1089/lap.2018.0392. Epub 2018 Jul 13. J Laparoendosc Adv Surg Tech A. 2018. PMID: 30004814 Review.
-
Decreased bleeding after laparoscopic sleeve gastrectomy with or without duodenal switch for morbid obesity using a stapled buttressed absorbable polymer membrane.Obes Surg. 2004 Nov-Dec;14(10):1360-6. doi: 10.1381/0960892042583905. Obes Surg. 2004. PMID: 15603652 Clinical Trial.
Cited by
-
Does intraoperative endoscopy decrease complications after bariatric surgery? Analysis of American College of Surgeons National Surgical Quality Improvement Program database.Surg Endosc. 2019 Nov;33(11):3629-3634. doi: 10.1007/s00464-018-06650-5. Epub 2019 Jan 31. Surg Endosc. 2019. PMID: 30706152
-
Gastric leaks after sleeve gastrectomy: a multicenter experience with 2,834 patients.Surg Endosc. 2013 Jan;27(1):240-5. doi: 10.1007/s00464-012-2426-x. Epub 2012 Jun 30. Surg Endosc. 2013. PMID: 22752283
-
Nonoperative Management Strategies for Anastomotic Leaks After One Anastomosis Gastric Bypass (OAGB): A Literature Review.Cureus. 2024 Sep 19;16(9):e69708. doi: 10.7759/cureus.69708. eCollection 2024 Sep. Cureus. 2024. PMID: 39429265 Free PMC article. Review.
-
Real-Time Perfusion and Leak Assessment in Bariatric Surgery: Bridging Traditional and Advanced Techniques.Cureus. 2024 Oct 20;16(10):e71919. doi: 10.7759/cureus.71919. eCollection 2024 Oct. Cureus. 2024. PMID: 39564049 Free PMC article. Review.
-
Reply to the Letter to the Editor Submitted by Michel Gagner (Publish with OBSU-D-15-00482).Obes Surg. 2016 Jan;26(1):151-3. doi: 10.1007/s11695-015-1901-6. Obes Surg. 2016. PMID: 26525979 No abstract available.
References
-
- Aggarwal S, Kini SU, Herron DM. Laparoscopic sleeve gastrectomy for morbid obesity: a review. Surg Obes Relat Dis. 2007;3:189–194. - PubMed
-
- Cottam D, Qureshi FG, Mattar SG, Sharma S, Holover S, Bonanomi G, Ramanathan R, Schauer P. Laparoscopic sleeve gastrectomy as an initial weight-loss procedure for high-risk patients with morbid obesity. Surg Endosc. 2006;20:859–863. - PubMed
-
- Deitel M, Crosby RD, Gagner M. The first international consensus summit for sleeve gastrectomy, New York City, October 25–27, 2007. Obes Surg. 2008;18:487–496. - PubMed
-
- Lalor PF, Tucker ON, Szomstein S, Rosenthal RJ. Complications after laparoscopic sleeve gastrectomy. Surg Obes Relat Dis. 2008;4:33–38. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
