

Echinocandin treatment of pneumocystis pneumonia in rodent models depletes cysts leaving trophic burdens that cannot transmit the infection
- PMID: 20126455
- PMCID: PMC2813285
- DOI: 10.1371/journal.pone.0008524
Echinocandin treatment of pneumocystis pneumonia in rodent models depletes cysts leaving trophic burdens that cannot transmit the infection
Abstract
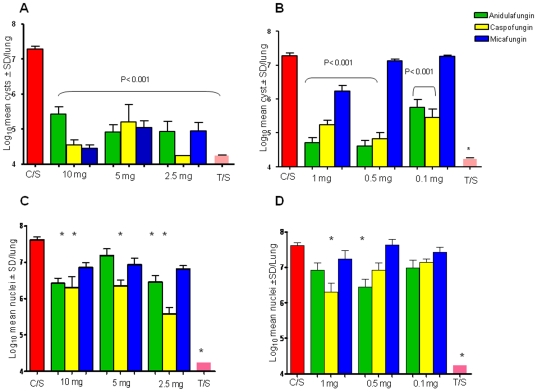
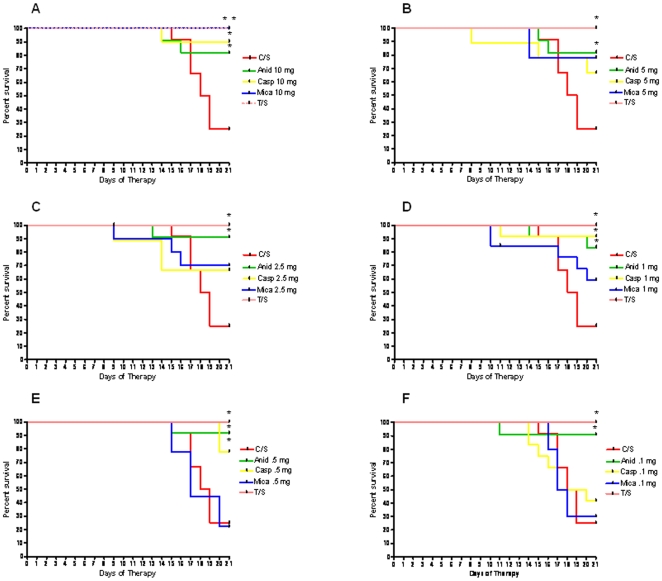
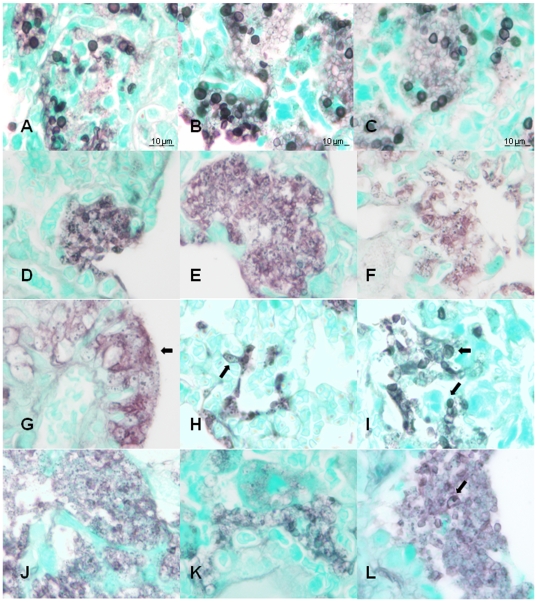
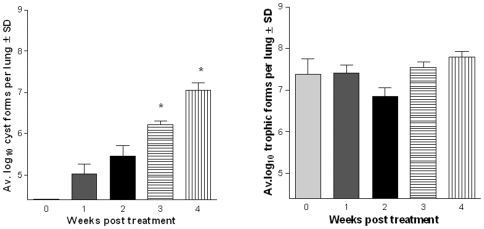
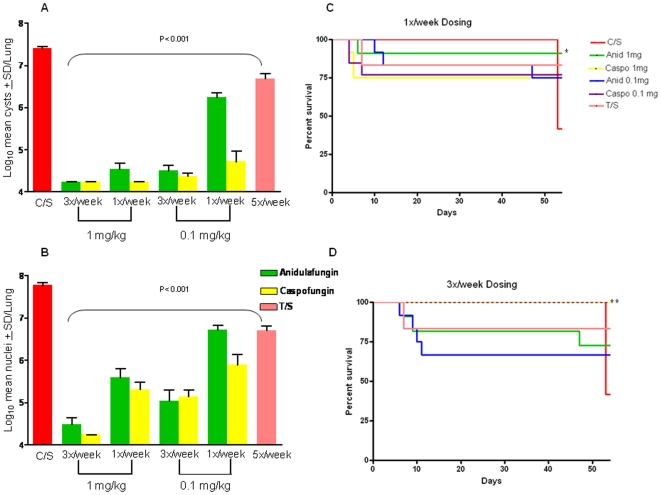
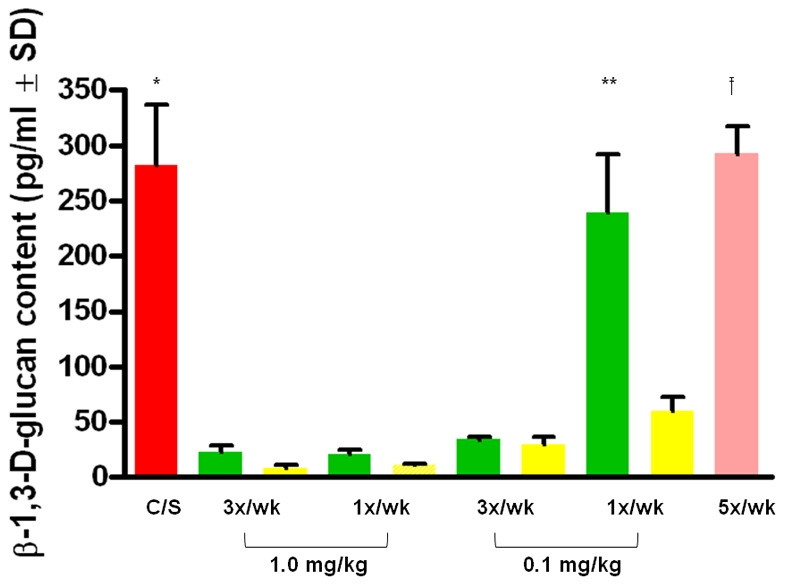
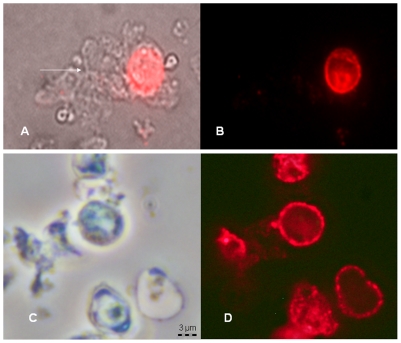
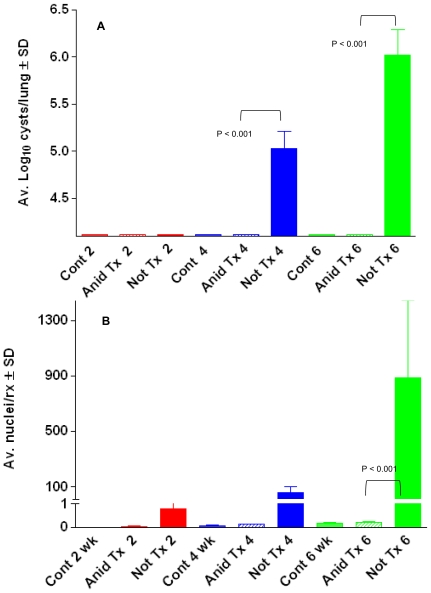
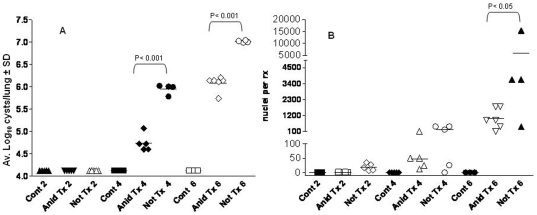
Fungi in the genus Pneumocystis cause pneumonia (PCP) in hosts with debilitated immune systems and are emerging as co-morbidity factors associated with chronic diseases such as COPD. Limited therapeutic choices and poor understanding of the life cycle are a result of the inability of these fungi to grow outside the mammalian lung. Within the alveolar lumen, Pneumocystis spp., appear to have a bi-phasic life cycle consisting of an asexual phase characterized by binary fission of trophic forms and a sexual cycle resulting in formation of cysts, but the life cycle stage that transmits the infection is not known. The cysts, but not the trophic forms, express beta -1,3-D-glucan synthetase and contain abundant beta -1,3-D-glucan. Here we show that therapeutic and prophylactic treatment of PCP with echinocandins, compounds which inhibit the synthesis of beta -1,3-D-glucan, depleted cysts in rodent models of PCP, while sparing the trophic forms which remained in significant numbers. Survival was enhanced in the echincandin treated mice, likely due to the decreased beta -1,3-D-glucan content in the lungs of treated mice and rats which coincided with reductions of cyst numbers, and dramatic remodeling of organism morphology. Strong evidence for the cyst as the agent of transmission was provided by the failure of anidulafungin-treated mice to transmit the infection. We show for the first time that withdrawal of anidulafungin treatment with continued immunosuppression permitted the repopulation of cyst forms. Treatment of PCP with an echinocandin alone will not likely result in eradication of infection and cessation of echinocandin treatment while the patient remains immunosuppressed could result in relapse. Importantly, the echinocandins provide novel and powerful chemical tools to probe the still poorly understood bi-phasic life cycle of this genus of fungal pathogens.
Conflict of interest statement
Figures
References
-
- Thomas CF, Jr, Limper AH. Current insights into the biology and pathogenesis of Pneumocystis pneumonia. Nat Rev Microbiol. 2007;5:298–308. - PubMed
-
- Vohra PK, Park JG, Sanyal B, Thomas CF., Jr Expression analysis of PCSTE3, a putative pheromone receptor from the lung pathogenic fungus Pneumocystis carinii. Biochem Biophys Res Commun. 2004;319:193–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
