

Three-dimensional nuclear telomere architecture is associated with differential time to progression and overall survival in glioblastoma patients
- PMID: 20126476
- PMCID: PMC2814356
- DOI: 10.1593/neo.91752
Three-dimensional nuclear telomere architecture is associated with differential time to progression and overall survival in glioblastoma patients
Abstract
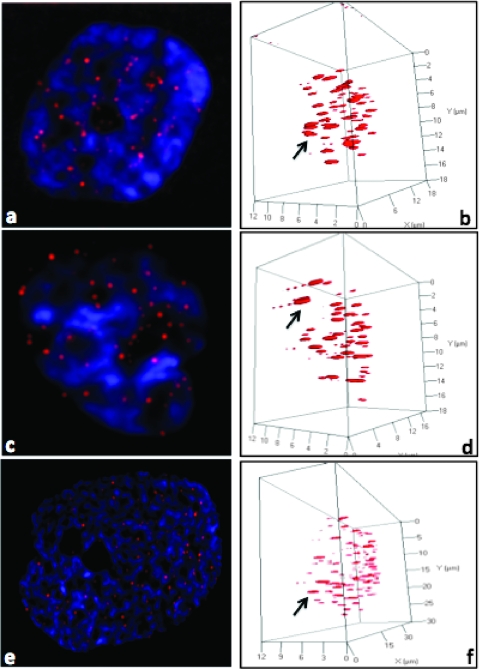
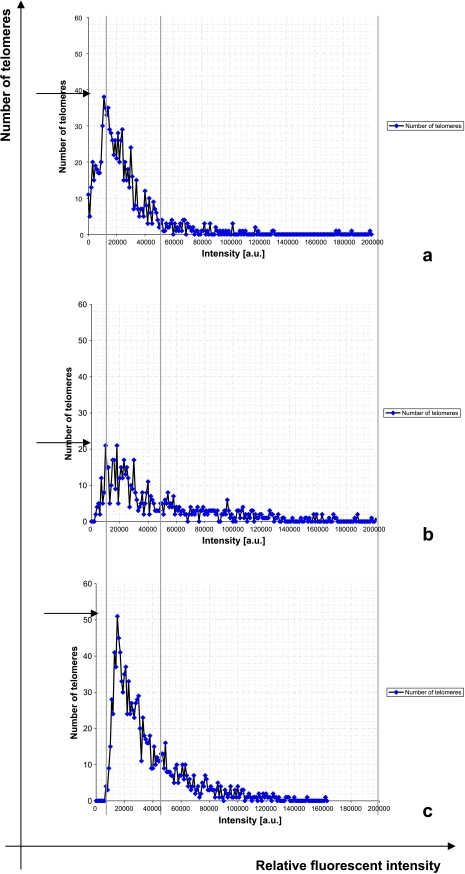
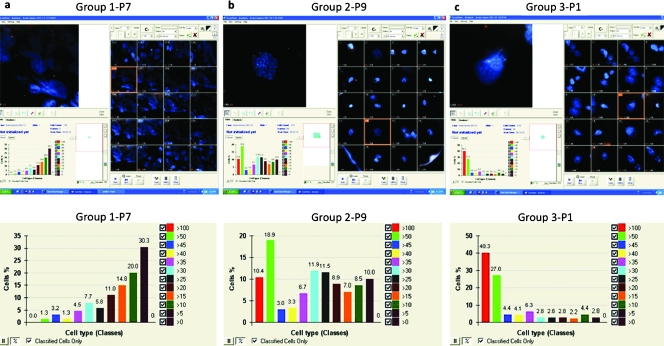
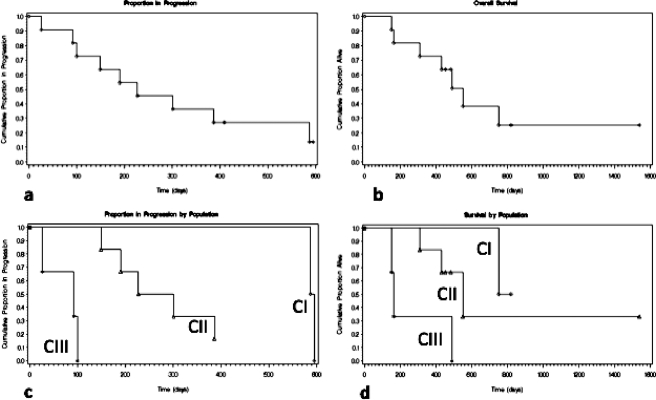
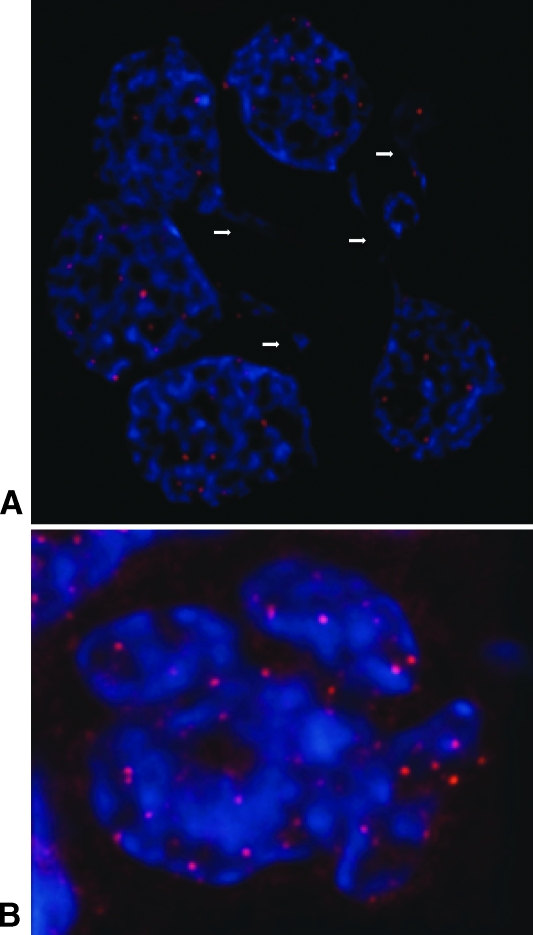
The absence of biological markers allowing for the assessment of the evolution and prognosis of glioblastoma (GBM) is a major impediment to the clinical management of GBM patients. The observed variability in patients' treatment responses and in outcomes implies biological heterogeneity and the existence of unidentified patient categories. Here, we define for the first time three GBM patient categories with distinct and clinically predictive three-dimensional nuclear-telomeric architecture defined by telomere number, size, and frequency of telomeric aggregates. GBM patient samples were examined by three-dimensional fluorescent in situ hybridization of telomeres using two independent three-dimensional telomere-measurement tools (TeloView program [P(1)] and SpotScan system [P(2)]). These measurements identified three patients categories (categories 1-3), displaying significant differences in telomere numbers/nucleus (P(1) = .0275; P(2) <or= .0001), telomere length (P(1) and P(2) = .0275), and number of telomeric aggregates (P(1) = .0464; P(2) <or= .0001). These categories corresponded to patients with long-term, intermediate, and short-term survival, respectively (P = .0393). The time to progression analyses showed significant differences between the three categories (P = .0167). There was a correlation between time to progression, median survival, and nuclear telomere architecture. Our study suggests a link between patient outcome and three-dimensional nuclear-telomere organization and highlights the potential clinical power of telomere signatures as a new prognostic, predictive, and potentially pharmacodynamic biomarker in GBM. Furthermore, novel automated three-dimensional high-throughput scanning as developed here permits to obtain data from 300 nuclei in 20 minutes. This method is applicable to any cell type and scanning application.
Figures
Similar articles
-
Three-Dimensional Nuclear Telomere Profiling as a Biomarker for Recurrence in Oligodendrogliomas: A Pilot Study.Int J Mol Sci. 2020 Nov 12;21(22):8539. doi: 10.3390/ijms21228539. Int J Mol Sci. 2020. PMID: 33198352 Free PMC article.
-
Profiling three-dimensional nuclear telomeric architecture of myelodysplastic syndromes and acute myeloid leukemia defines patient subgroups.Clin Cancer Res. 2012 Jun 15;18(12):3293-304. doi: 10.1158/1078-0432.CCR-12-0087. Epub 2012 Apr 26. Clin Cancer Res. 2012. PMID: 22539801
-
Novel automated three-dimensional genome scanning based on the nuclear architecture of telomeres.Cytometry A. 2011 Feb;79(2):159-66. doi: 10.1002/cyto.a.21012. Epub 2010 Dec 30. Cytometry A. 2011. PMID: 21265009
-
Influence of glioblastoma contact with the lateral ventricle on survival: a meta-analysis.J Neurooncol. 2017 Jan;131(1):125-133. doi: 10.1007/s11060-016-2278-7. Epub 2016 Sep 19. J Neurooncol. 2017. PMID: 27644688 Free PMC article. Review.
-
Nuclear imaging in three dimensions: a unique tool in cancer research.Ann Anat. 2010 Sep 20;192(5):292-301. doi: 10.1016/j.aanat.2010.07.007. Epub 2010 Aug 6. Ann Anat. 2010. PMID: 20800459 Review.
Cited by
-
The interconnectedness of cancer cell signaling.Neoplasia. 2011 Dec;13(12):1183-93. doi: 10.1593/neo.111746. Neoplasia. 2011. PMID: 22241964 Free PMC article.
-
Transforming growth factor-beta and its implication in the malignancy of gliomas.Target Oncol. 2015 Mar;10(1):1-14. doi: 10.1007/s11523-014-0308-y. Epub 2014 Mar 5. Target Oncol. 2015. PMID: 24590691 Review.
-
p53 CRISPR Deletion Affects DNA Structure and Nuclear Architecture.J Clin Med. 2020 Feb 22;9(2):598. doi: 10.3390/jcm9020598. J Clin Med. 2020. PMID: 32098416 Free PMC article.
-
3D Telomere Structure Analysis to DetectGenomic Instability and Cytogenetic Evolutionin Myelodysplastic Syndromes.Cells. 2019 Apr 2;8(4):304. doi: 10.3390/cells8040304. Cells. 2019. PMID: 30987070 Free PMC article.
-
Advancing Risk Assessment of Intermediate Risk Prostate Cancer Patients.Cancers (Basel). 2019 Jun 20;11(6):855. doi: 10.3390/cancers11060855. Cancers (Basel). 2019. PMID: 31226731 Free PMC article.
References
-
- Louis DN, Pomeroy SL, Cairncross JG. Focus on central nervous system neoplasia. Cancer Cell. 2002;1:125–128. - PubMed
-
- Krex D, Klink B, Hartmann C, von Deimling A, Pietsch T, Simon M, Sabel M, Steinbach JP, Heese O, Reifenberger G, et al. Long-term survival with glioblastoma multiforme. Brain. 2007;130:2596–2606. - PubMed
-
- Furnari FB, Fenton T, Bachoo RM, Mukasa A, Stommel JM, Stegh A, Hahn WC, Ligon KL, Louis DN, Brennan C, et al. Malignant astrocytic glioma: genetics, biology, and paths to treatment. Genes Dev. 2007;21:2683–2710. - PubMed
-
- Wen PY, Kesari S. Malignant gliomas in adults. N Engl J Med. 2008;359:492–507. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical