

Inferior oblique surgery for restrictive strabismus in patients with thyroid orbitopathy
- PMID: 20126484
- PMCID: PMC2814581
Inferior oblique surgery for restrictive strabismus in patients with thyroid orbitopathy
Abstract
Introduction: Thyroid orbitopathy is the most common cause of restrictive strabismus. Patients often present with vertical or horizontal double vision, or both, due to restriction involving most commonly the inferior and medial rectus muscles. Traditional muscle surgery involves release of the tight muscles. Previous literature has described a frequent need for secondary operations and an overcorrection incidence of up to 50%. Recognizing that the tight muscles are also limited in their excursion, it was proposed that operating on the better-moving eye, particularly the inferior oblique, might produce an improvement in binocularity and decrease the incidence of overcorrection.
Methods: A total of 37 patients with restrictive strabismus due to thyroid orbitopathy treated at the University of Virginia over 12 years with inferior oblique surgery were retrospectively reviewed.
Results: Eight patients were treated with a combination of inferior oblique surgery and horizontal muscle surgery at the same time. One patient was treated with simultaneous inferior oblique and superior rectus surgery. Seven patients had vertical correction with inferior oblique surgery alone. Twenty-three patients required secondary procedures. Eight patients were overcorrected but only one following primary surgery. At the time of last follow-up, ranging from 6 months to 8 years, 33 patients had no diplopia, 2 had minimal diplopia, and 2 had persistent diplopia. All but two were completely functional.
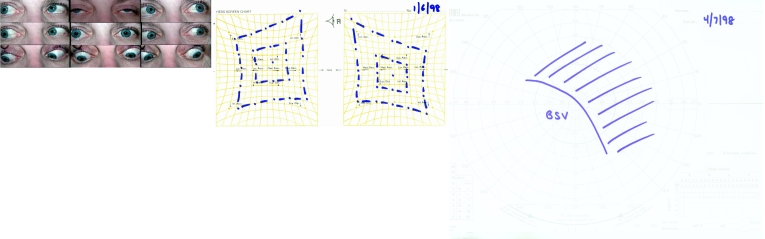
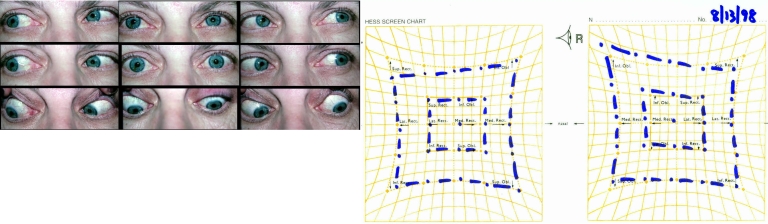
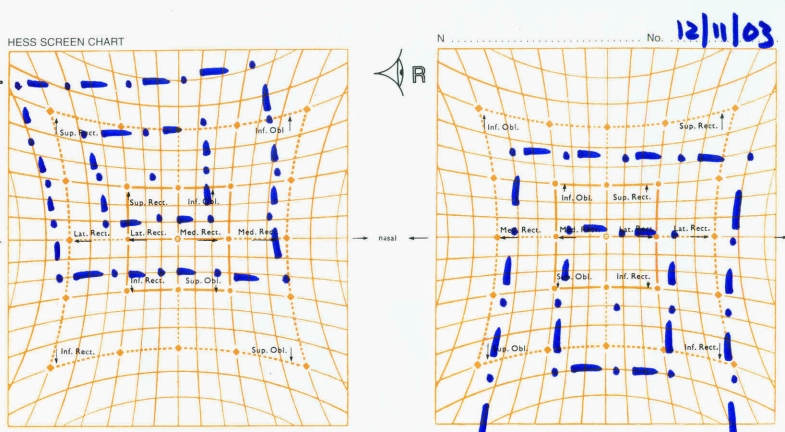
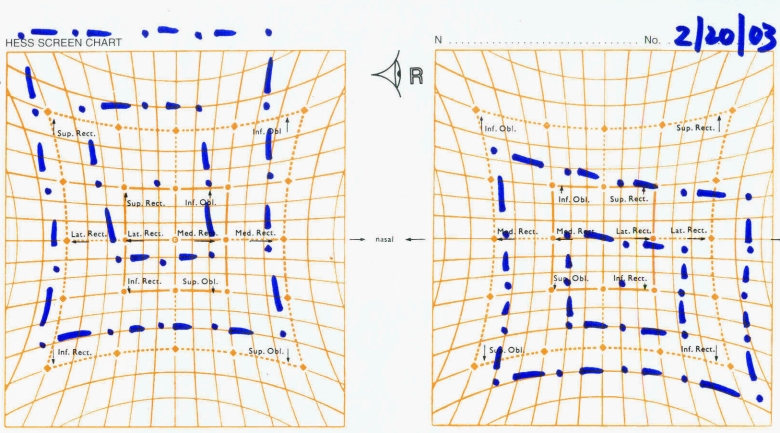
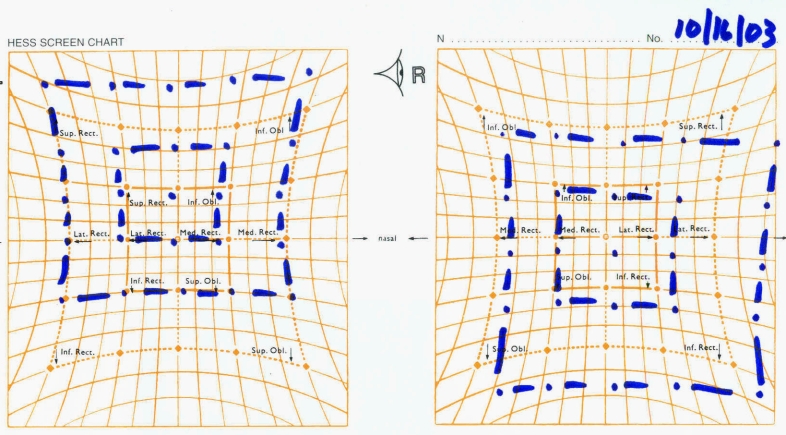
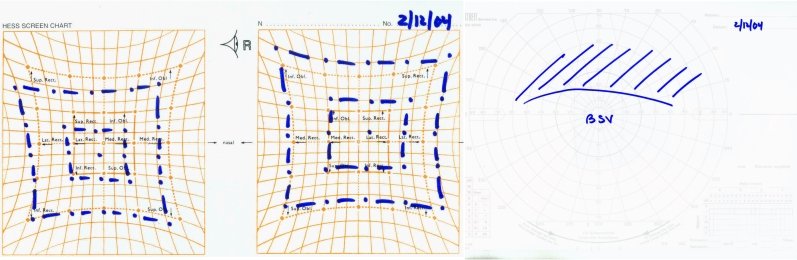
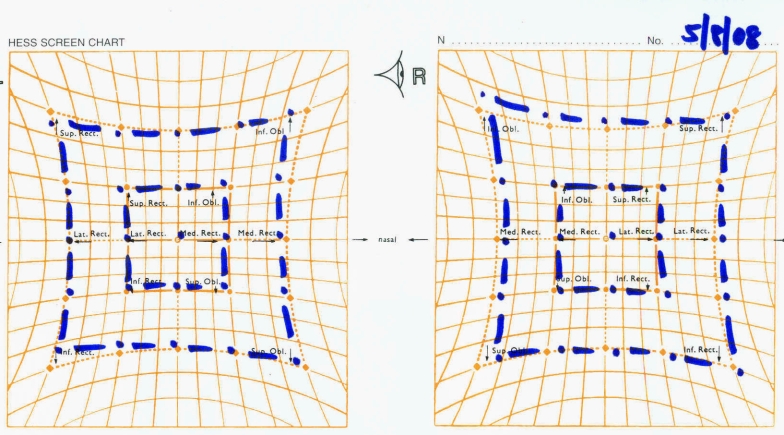
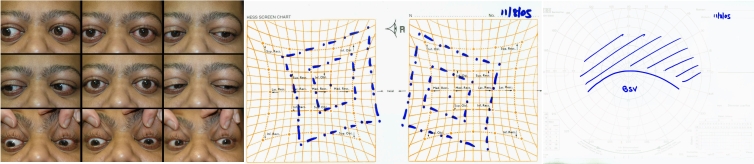
Conclusion: Inferior oblique surgery by balancing the overall excursion of extraocular muscles in thyroid patients may produce binocularity in primary position and down reading gaze. The amount of vertical correction from inferior oblique surgery alone is limited, often requiring ipsilateral superior or contralateral inferior rectus surgery. Inferior oblique surgery likely increases the area of binocular single vision and decreases the incidence of overcorrection. The use of Hess screen and binocular single vision fields is helpful in assessment and planning of surgery in these patients.
Figures
















References
-
- Bok C, Hidalgo C, Morax S. Surgical management of diplopia in dysthyroid orbitopathy. J Fr Ophtamol. 2007;30:390–396. - PubMed
-
- Chu YK, Kim SJ, Lee SY. Surgical treatment modalities of thyroid ophthalmopathy. Korean J Ophthalmol. 2001;15:128–132. - PubMed
-
- Looi ALG, Luu CD, Wong TY, Seah LL, Rootman J. Factors associated with decompression and strabismus surgery in thyroid eye disease. Ann Acad Med Singapore. 2005;34:154–157. - PubMed
-
- Garrity JA, Fatourechi V, Bergstralh V, et al. Results of transantral orbital decompression in 428 patients with severe Graves’ orbitopathy. Am J Ophthalmol. 1993;116:533–547. - PubMed
-
- Werner SC, Coleman DJ, Franzen LA. Ultrasonographic evidence of a consistent orbital involvement in Graves’ disease. N Engl J Med. 1974;290:1447–1450. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
