

Cost modeling of preoperative axillary ultrasound and fine-needle aspiration to guide surgery for invasive breast cancer
- PMID: 20127185
- PMCID: PMC2908087
- DOI: 10.1245/s10434-010-0919-1
Cost modeling of preoperative axillary ultrasound and fine-needle aspiration to guide surgery for invasive breast cancer
Abstract
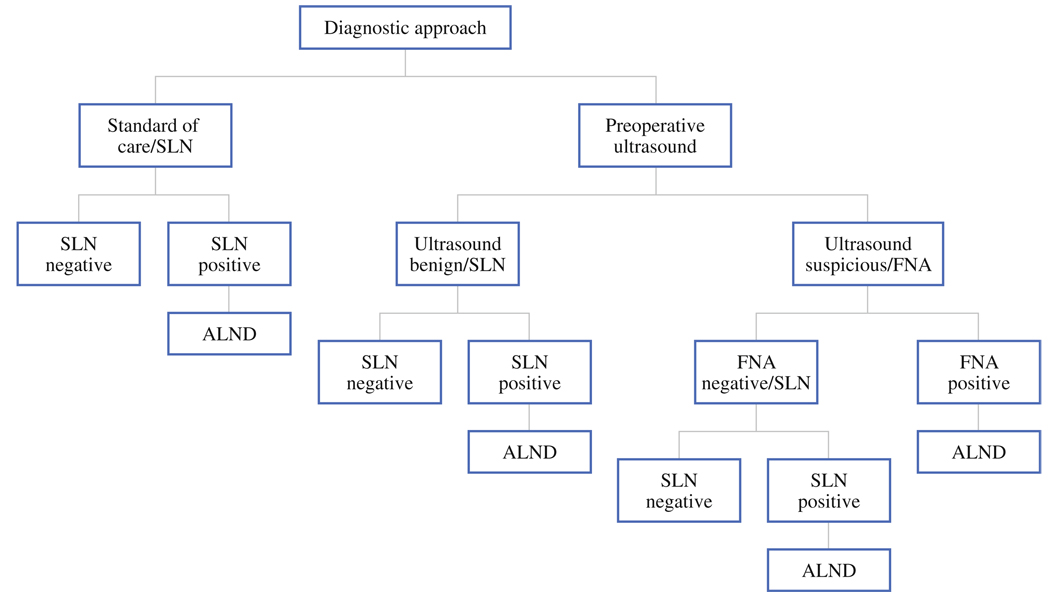
Purpose: Preoperative axillary lymph node ultrasound (US) and fine-needle aspiration (FNA) biopsy can identify a proportion of node-positive patients and avoid sentinel lymph node (SLN) surgery and direct surgical treatment. We compared the costs with preoperative US/FNA to without US/FNA (standard of care) for invasive breast cancer.
Methods: Using decision-analytic software we constructed a model to assess the costs associated with the two preoperative strategies. Diagnostic test sensitivities and specificities were obtained from literature review. Costs were derived from Medicare payment rates and actual resource utilization. Base-case results were fully probabilistic to capture parameter uncertainty in economic results.
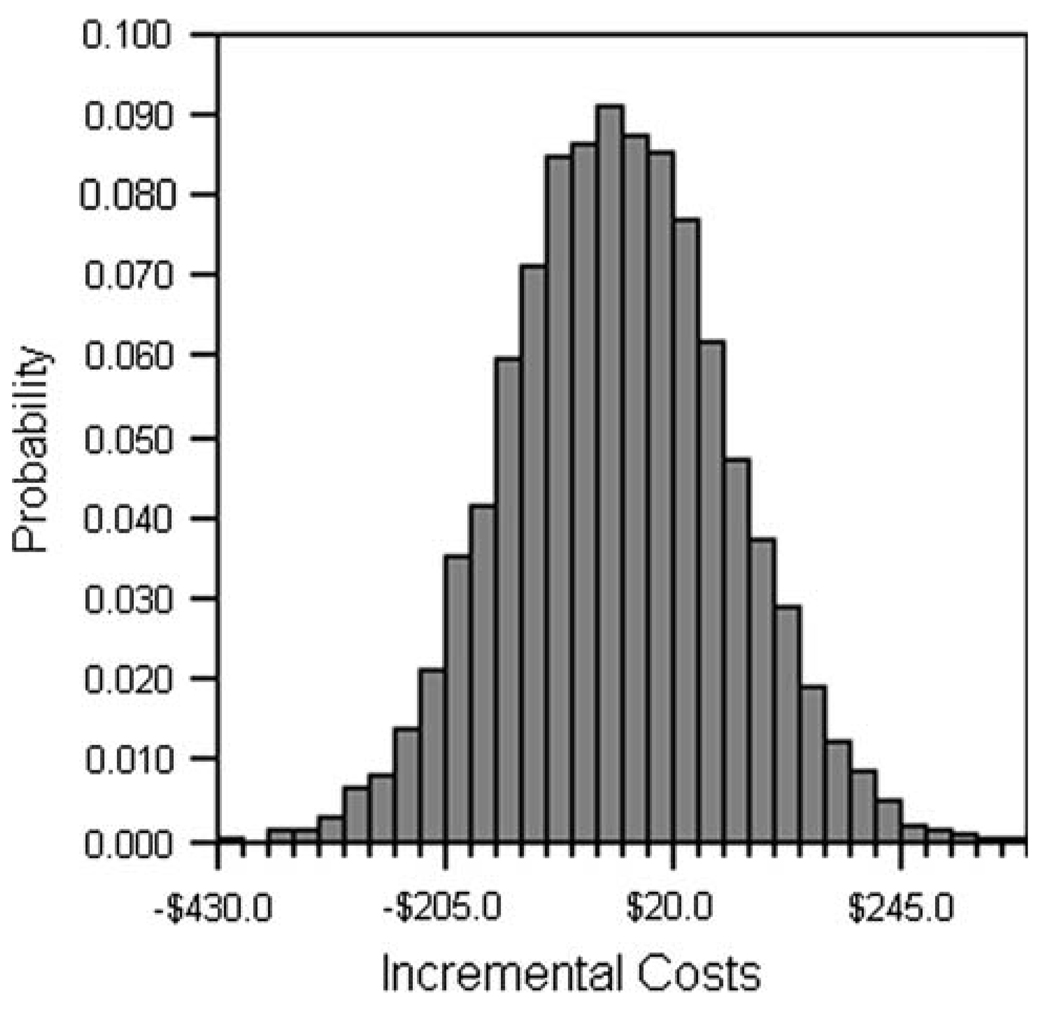
Results: Base-case results estimate total mean costs per patient of $10,947 ("$" indicates US dollars throughout) with the US/FNA strategy and $10,983 with standard of care, an incremental cost savings of $36, on average, per patient [95% confidence interval (CI) of cost difference: -$248 to $179]. Most (63%) of the simulations resulted in cost saving with axillary US/FNA. One-way sensitivity analyses suggest that results are sensitive to assumed diagnostic and surgical costs and selected diagnostic test parameters. US/FNA approach was similar in costs or cost saving relative to the standard of care for all tumor stages.
Conclusions: The additional cost of performing axillary US with possible FNA in every patient is balanced, on average, by the savings from avoiding SLN in cases where metastasis can be documented preoperatively. Routine use of preoperative axillary US with FNA to guide surgical planning can decrease the overall cost of patient care for invasive breast cancer.
Figures
Similar articles
-
Selective application of routine preoperative axillary ultrasonography reduces costs for invasive breast cancers.Oncologist. 2011;16(7):942-8. doi: 10.1634/theoncologist.2010-0373. Epub 2011 May 14. Oncologist. 2011. PMID: 21572122 Free PMC article.
-
Cost/accuracy ratio analysis in breast cancer patients undergoing ultrasound-guided fine-needle aspiration cytology, sentinel node biopsy, and frozen section of node.World J Surg. 2007 Jun;31(6):1155-63. doi: 10.1007/s00268-007-9009-3. World J Surg. 2007. PMID: 17464539
-
Impact of preoperative ultrasonography and fine-needle aspiration of axillary lymph nodes on surgical management of primary breast cancer.Ann Surg Oncol. 2011 Mar;18(3):738-44. doi: 10.1245/s10434-010-1347-y. Epub 2010 Oct 2. Ann Surg Oncol. 2011. PMID: 20890729 Clinical Trial.
-
Meta-analysis of the diagnostic accuracy of ultrasound-guided fine-needle aspiration and core needle biopsy in diagnosing axillary lymph node metastasis.Br J Surg. 2018 Sep;105(10):1244-1253. doi: 10.1002/bjs.10920. Epub 2018 Jul 4. Br J Surg. 2018. PMID: 29972239
-
Accuracy of axillary ultrasound in the diagnosis of nodal metastasis in invasive breast cancer: a review.World J Surg. 2012 Jan;36(1):46-54. doi: 10.1007/s00268-011-1319-9. World J Surg. 2012. PMID: 22037691 Review.
Cited by
-
Development and validation of a radiogenomics model to predict axillary lymph node metastasis in breast cancer integrating MRI with transcriptome data: A multicohort study.Front Oncol. 2022 Dec 29;12:1076267. doi: 10.3389/fonc.2022.1076267. eCollection 2022. Front Oncol. 2022. PMID: 36644636 Free PMC article.
-
Breast cancer: comparison of quantitative dual-layer spectral CT and axillary ultrasonography for preoperative diagnosis of metastatic axillary lymph nodes.Eur Radiol Exp. 2021 Apr 9;5(1):16. doi: 10.1186/s41747-021-00212-6. Eur Radiol Exp. 2021. PMID: 33834317 Free PMC article.
-
Ultrasound derived deep learning features for predicting axillary lymph node metastasis in breast cancer using graph convolutional networks in a multicenter study.Sci Rep. 2025 Jul 30;15(1):27796. doi: 10.1038/s41598-025-13086-0. Sci Rep. 2025. PMID: 40738938 Free PMC article.
-
Specimen number based diagnostic yields of suspicious axillary lymph nodes in core biopsy in breast cancer: clinical implications from a prospective exploratory study.Quant Imaging Med Surg. 2021 May;11(5):2151-2161. doi: 10.21037/qims-20-1030. Quant Imaging Med Surg. 2021. PMID: 33936995 Free PMC article.
-
Deep learning radiomics for prediction of axillary lymph node metastasis in patients with clinical stage T1-2 breast cancer.Quant Imaging Med Surg. 2023 Aug 1;13(8):4995-5011. doi: 10.21037/qims-22-1257. Epub 2023 Jun 8. Quant Imaging Med Surg. 2023. PMID: 37581073 Free PMC article.
References
-
- Mathijssen IMJ, Strijdhorst H, Kiestra SK, et al. Added value of ultrasound in screening the clinically negative axilla in breast cancer. J Surg Oncol. 2006;94:364–367. - PubMed
-
- van Rijk MC, Deurloo EE, Nieweg OE, et al. Ultrasonography and fine-needle aspiration cytology can spare breast cancer patients unnecessary sentinel lymph node biopsy. Ann Surg Oncol. 2006;13:31–35. - PubMed
-
- Deurloo EE, Tanis PJ, Gilhuijs KGA, et al. Reduction in the number of sentinel lymph node procedures by preoperative ultrasonography of the axilla in breast cancer. Eur J Cancer. 2003;39:1068–1073. - PubMed
-
- Krishnamurthy S, Sneige N, Bedi DG, et al. Role of ultrasound-guided fine-needle aspiration of indeterminate and suspicious axillary lymph nodes in the initial staging of breast carcinoma. Cancer. 2002;95:982–988. - PubMed
-
- Genta F, Zanon E, Camanni M, et al. Cost/accuracy ratio analysis in breast cancer patients undergoing ultrasound-guided fine-needle aspiration cytology, sentinel node biopsy, and frozen section of node. World J Surg. 2007;31:1155–1163. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
