

Comparative performance of gene-based warfarin dosing algorithms in a multiethnic population
- PMID: 20128861
- PMCID: PMC4441275
- DOI: 10.1111/j.1538-7836.2010.03792.x
Comparative performance of gene-based warfarin dosing algorithms in a multiethnic population
Abstract
Summary background: Gene-based warfarin dosing algorithms have largely been developed in homogeneous populations, and their generalizability has not been established.
Objectives: We sought to assess the performance of published algorithms in a racially diverse and multiethnic sample, and determine if additional clinical variables or genetic variants associated with dose could enhance algorithm performance.
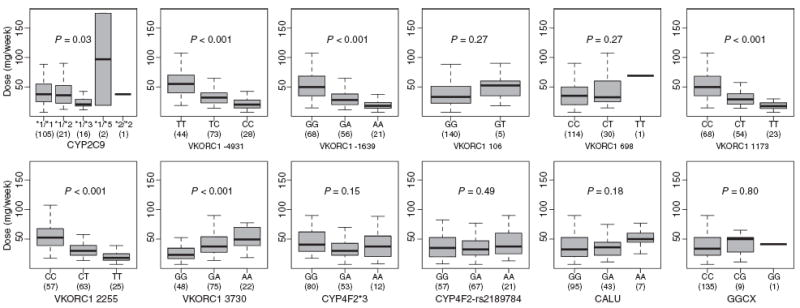
Patients and methods: In 145 compliant patients on warfarin with a goal international normalized ratio (INR) of 2-3, stable, therapeutic doses were compared with predicted doses using 12 reported algorithms that incorporated CYP2C9 and VKORC1 variants. Additional covariates tested with each model included race, concurrent medications, medications known to interact with warfarin and previously described CYP4F2, CALU and GGCX variants.
Results: The mean patient age was 67 +/- 14 years; 90 (62%) were male. Eighty-two (57%) were Caucasian, 28 (19%) African-American, 20 (14%) Hispanic and 15 (10%) Asian. The median warfarin dose was 35 mg per week (interquartile range 23-53 mg per week). Gene-based dosing algorithms explained 37-55% of the variation in warfarin dose requirements. Neither the addition of race, number of concurrent medications nor the number of concurrent medications interacting with warfarin enhanced algorithm performance. Similarly, consideration of CYP4F2, CALU or GGCX variant genotypes did not improve algorithms.
Conclusions: Existing gene-based dosing algorithms explained between approximately one-third and one-half of the variability in warfarin dose requirements in this racially and ethnically diverse cohort. Additional clinical and recently described genetic variants associated with warfarin dose did not enhance prediction in our patient population.
Conflict of interest statement
The authors state that they have no conflict of interest.
Figures

References
-
- Hirsh J, Fuster V, Ansell J, Halperin JL. American Heart Association/American College of Cardiology Foundation guide to warfarin therapy. J Am Coll Cardiol. 2003;41:1633–52. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
