

Self-reported physical and mental health status and quality of life in adolescents: a latent variable mediation model
- PMID: 20128913
- PMCID: PMC2829530
- DOI: 10.1186/1477-7525-8-17
Self-reported physical and mental health status and quality of life in adolescents: a latent variable mediation model
Abstract
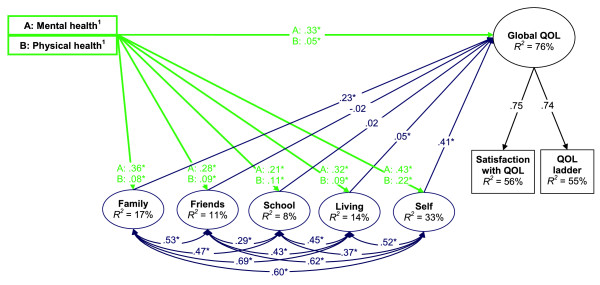
Background: We examined adolescents' differentiation of their self-reported physical and mental health status, the relative importance of these variables and five important life domains (satisfaction with family, friends, living environment, school and self) with respect to adolescents' global quality of life (QOL), and the extent to which the five life domains mediate the relationships between self-reported physical and mental health status and global QOL.
Methods: The data were obtained via a cross-sectional health survey of 8,225 adolescents in 49 schools in British Columbia, Canada. Structural equation modeling was applied to test the implied latent variable mediation model. The Pratt index (d) was used to evaluate variable importance.
Results: Relative to one another, self-reported mental health status was found to be more strongly associated with depressive symptoms, and self-reported physical health status more strongly associated with physical activity. Self-reported physical and mental health status and the five life domains explained 76% of the variance in global QOL. Relatively poorer mental health and physical health were significantly associated with lower satisfaction in each of the life domains. Global QOL was predominantly explained by three of the variables: mental health status (d = 30%), satisfaction with self (d = 42%), and satisfaction with family (d = 20%). Satisfaction with self and family were the predominant mediators of mental health and global QOL (45% total mediation), and of physical health and global QOL (68% total mediation).
Conclusions: This study provides support for the validity and relevance of differentiating self-reported physical and mental health status in adolescent health surveys. Self-reported mental health status and, to a lesser extent, self-reported physical health status were associated with significant differences in the adolescents' satisfaction with their family, friends, living environment, school experiences, self, and their global QOL. Questions about adolescents' self-reported physical and mental health status and their experiences with these life domains require more research attention so as to target appropriate supportive services, particularly for adolescents with mental or physical health challenges.
Figures
Similar articles
-
Adolescent distinctions between quality of life and self-rated health in quality of life research.Health Qual Life Outcomes. 2005 Oct 25;3:64. doi: 10.1186/1477-7525-3-64. Health Qual Life Outcomes. 2005. PMID: 16248897 Free PMC article.
-
Self- and proxy reports of quality of life among adolescents living in residential youth care compared to adolescents in the general population and mental health services.Health Qual Life Outcomes. 2015 Jul 22;13:104. doi: 10.1186/s12955-015-0280-y. Health Qual Life Outcomes. 2015. PMID: 26197764 Free PMC article.
-
Comparing immigrant children with native Greek in self-reported-Quality of Life.Psychiatriki. 2016 Jan-Mar;27(1):37-43. Psychiatriki. 2016. PMID: 27110881
-
Quality-of-life measures in chronic diseases of childhood.Health Technol Assess. 2001;5(4):1-157. doi: 10.3310/hta5040. Health Technol Assess. 2001. PMID: 11262421 Review.
-
The importance of quality of life in patients with alcohol abuse and dependence.Harv Rev Psychiatry. 2013 Jan-Feb;21(1):1-17. doi: 10.1097/HRP.0b013e31827fd8aa. Harv Rev Psychiatry. 2013. PMID: 23656759 Review.
Cited by
-
Efficacy-mediated effects of spirituality and physical activity on quality of life: a path analysis.Health Qual Life Outcomes. 2012 May 29;10:57. doi: 10.1186/1477-7525-10-57. Health Qual Life Outcomes. 2012. PMID: 22642832 Free PMC article.
-
Construct and Psychometric Properties of a New Version Quality of Life Scale Based on Choice Theory.Open Access Maced J Med Sci. 2019 Feb 11;7(3):440-445. doi: 10.3889/oamjms.2019.075. eCollection 2019 Feb 15. Open Access Maced J Med Sci. 2019. PMID: 30834017 Free PMC article.
-
Mental health problems among healthcare professionals following the workplace violence issue-mediating effect of risk perception.Front Psychol. 2022 Aug 31;13:971102. doi: 10.3389/fpsyg.2022.971102. eCollection 2022. Front Psychol. 2022. PMID: 36160531 Free PMC article.
-
Bilingualism: A Pearl to Overcome Certain Perils of Cochlear Implants.J Med Speech Lang Pathol. 2014;21(2):107-125. J Med Speech Lang Pathol. 2014. PMID: 25419095 Free PMC article.
-
Migraine Attacks and Relevant Trigger Factors in Undergraduate Nursing Students in Hong Kong: A Cross-Sectional Study.J Pain Res. 2022 Mar 10;15:701-713. doi: 10.2147/JPR.S337465. eCollection 2022. J Pain Res. 2022. PMID: 35300404 Free PMC article.
References
-
- Kaplan RM. In: Measuring Health-Related Quality of Life in Children and Adolescents. Drotar D, editor. Mahwah, NJ: Lawrence Erlbaum; 1998. Implication of quality of life assessment in public policy for adolescent health; pp. 63–84.
-
- Raphael D, Brown I, Rukholm E, Hill-Bailey P. Adolescent health: moving from prevention to promotion through a quality of life approach. Can J Public Health. 1996;87:81–83. - PubMed
-
- Dannerbeck A, Casas F, Sadurni M, Coenders G. Quality-of-Life Research on Children and Adolescents. Dordrecht, Netherlands: Kluwer; 2004.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
