

Preferences versus practice: life-sustaining treatments in last months of life in long-term care
- PMID: 20129214
- PMCID: PMC3692740
- DOI: 10.1016/j.jamda.2009.07.005
Preferences versus practice: life-sustaining treatments in last months of life in long-term care
Abstract
Purpose: To determine prevalence and correlates of decisions made about specific life-sustaining treatments (LSTs) among residents in long-term care (LTC) settings, including characteristics associated with having an LST performed when the resident reportedly did not desire the LST.
Design and participants: After-death interviews with 1 family caregiver and 1 staff caregiver for each of 327 LTC residents who died in the facility.
Setting: The setting included 27 nursing homes (NHs) and 85 residential care/assisted living (RC/AL) settings in 4 states.
Measurements: Decedent demographics, facility characteristics, prevalence of decisions made about specific LSTs, percentage of time LSTs were performed when reportedly not desired, and characteristics associated with that.
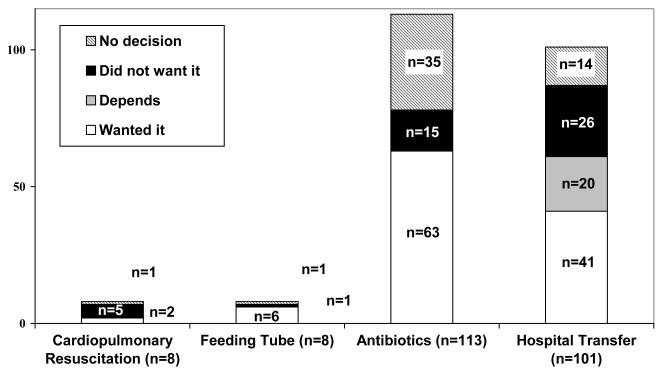
Results: Most family caregivers reported making a decision with a physician about resuscitation (89.1%), inserting a feeding tube (82.1%), administering antibiotics (64.3%), and hospital transfer (83.7%). Reported care was inconsistent with decisions made in 5 of 7 (71.4%) resuscitations, 1 of 7 feeding tube insertions (14.3%), 15 of 78 antibiotics courses (19.2%), and 26 of 87 hospital transfers (29.9%). Decedents who received antibiotics contrary to their wishes were older (mean age 92 versus 85, P=.014). More than half (53.8%) of decedents who had care discordant with their wishes about hospitalization lived in a NH compared with 32.8% of those whose decisions were concordant (P=.034).
Conclusion: Most respondents reported decision making with a doctor about life-sustaining treatments, but those decisions were not consistently heeded. Being older and living in a NH were risk factors for decisions not being heeded.
Copyright (c) 2010 American Medical Directors Association. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Disparities between preferences and practice for end-of-life care.J Am Med Dir Assoc. 2010 Jan;11(1):9-10. doi: 10.1016/j.jamda.2009.09.010. Epub 2009 Nov 25. J Am Med Dir Assoc. 2010. PMID: 20129208 No abstract available.
Similar articles
-
Advance care planning in nursing homes and assisted living communities.J Am Med Dir Assoc. 2009 May;10(4):243-51. doi: 10.1016/j.jamda.2008.10.015. Epub 2009 Mar 28. J Am Med Dir Assoc. 2009. PMID: 19426940 Free PMC article.
-
Terminally Ill Taiwanese Cancer Patients' and Family Caregivers' Agreement on Patterns of Life-Sustaining Treatment Preferences Is Poor to Fair and Declines Over a Decade: Results From Two Independent Cross-Sectional Studies.J Pain Symptom Manage. 2017 Jul;54(1):35-45.e4. doi: 10.1016/j.jpainsymman.2017.02.013. Epub 2017 Apr 24. J Pain Symptom Manage. 2017. PMID: 28450219
-
End-of-life care in assisted living and related residential care settings: comparison with nursing homes.J Am Geriatr Soc. 2003 Nov;51(11):1587-94. doi: 10.1046/j.1532-5415.2003.51511.x. J Am Geriatr Soc. 2003. PMID: 14687388
-
Should I hospitalize my resident with nursing home-acquired pneumonia?J Am Med Dir Assoc. 2005 Sep-Oct;6(5):327-33. doi: 10.1016/j.jamda.2005.06.005. J Am Med Dir Assoc. 2005. PMID: 16165074 Review.
-
Experiences and involvement of family members in transfer decisions from nursing home to hospital: a systematic review of qualitative research.BMC Geriatr. 2019 Jun 4;19(1):155. doi: 10.1186/s12877-019-1170-7. BMC Geriatr. 2019. PMID: 31164101 Free PMC article.
Cited by
-
Conceptualizing and Counting Discretionary Utilization in the Final 100 Days of Life: A Scoping Review.J Pain Symptom Manage. 2020 Apr;59(4):894-915.e14. doi: 10.1016/j.jpainsymman.2019.10.009. Epub 2019 Oct 19. J Pain Symptom Manage. 2020. PMID: 31639495 Free PMC article.
-
Attitudes toward withholding antibiotics from people with dementia lacking decisional capacity: findings from a survey of Canadian stakeholders.BMC Med Ethics. 2021 Sep 6;22(1):119. doi: 10.1186/s12910-021-00689-1. BMC Med Ethics. 2021. PMID: 34488722 Free PMC article.
-
Palliative care for persons with late-stage Alzheimer's and related dementias and their caregivers: protocol for a randomized clinical trial.Trials. 2023 Sep 25;24(1):606. doi: 10.1186/s13063-023-07614-4. Trials. 2023. PMID: 37743478 Free PMC article.
-
Barriers to the composition and implementation of advance directives in oncology: a literature review.Ecancermedicalscience. 2019 Nov 12;13:974. doi: 10.3332/ecancer.2019.974. eCollection 2019. Ecancermedicalscience. 2019. PMID: 31921345 Free PMC article. Review.
-
Advance Directives and Care Received by Older Nursing Home Residents.Am J Hosp Palliat Care. 2017 Mar;34(2):105-110. doi: 10.1177/1049909115611875. Epub 2016 Jul 11. Am J Hosp Palliat Care. 2017. PMID: 26494830 Free PMC article.
References
-
- Braun KL, Karel H, Zir A. Family Response to End-of-Life Education: Differences by Ethnicity and Stage of Caregiving. American Journal of Hospice and Palliative Medicine. 2006;23:269–276. - PubMed
-
- Brock DB, Foley DJ. Demography and epidemiology of dying in the U.S. with emphasis on deaths of older persons. Hospice Journal. 1998;13(1-2):49–60. - PubMed
-
- Cartwright JC. Nursing homes and assisted living facilities as places for dying. Annual Review of Nursing Research. 2002;20:231–264. - PubMed
-
- Culberson J, Levy C, Lawhorne L. Do not hospitalize orders in nursing homes: A pilot study. Journal of the American Medical Directors Association. 2005;6(1):22–26. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
