

Mechanisms that initiate ventricular tachycardia in the infarcted human heart
- PMID: 20129286
- PMCID: PMC2806968
- DOI: 10.1016/j.hrthm.2009.09.025
Mechanisms that initiate ventricular tachycardia in the infarcted human heart
Abstract
Background: Precise mechanisms that initiate ventricular tachycardia (VT) in the intact infarcted human heart have not been defined.
Objective: The purpose of this study was to investigate the mechanisms that underlie human postinfarct VT initiation.
Methods: Noncontact mapping of the left ventricle was performed in 9 patients (age 67.1 +/- 7.8 years, ejection fraction 34.4% +/- 5%) with previous myocardial infarction and sustained monomorphic VT.
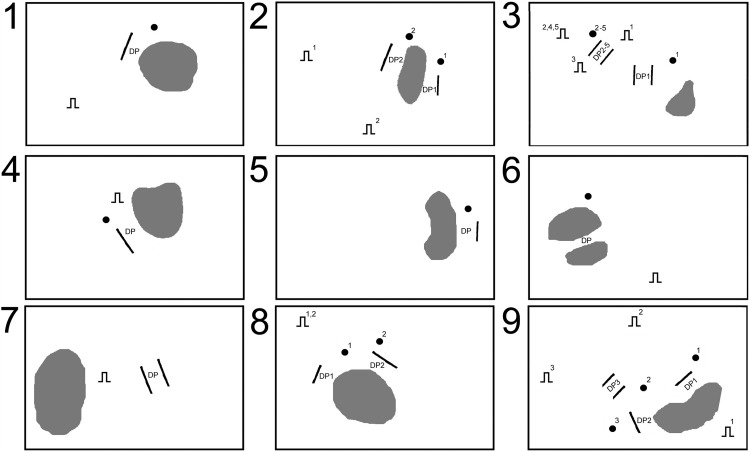
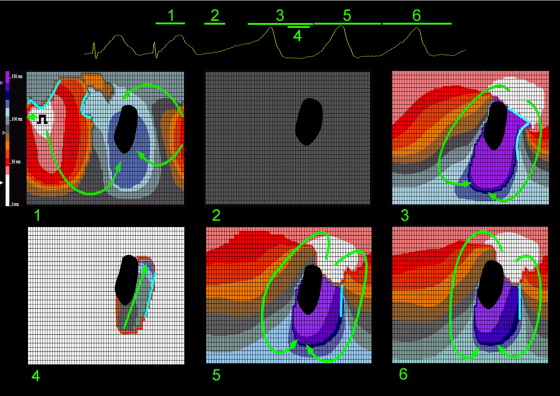
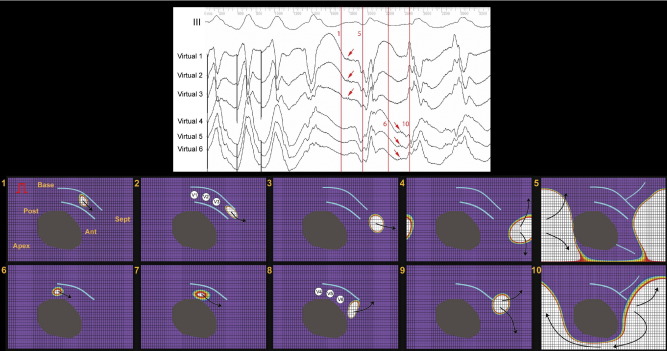
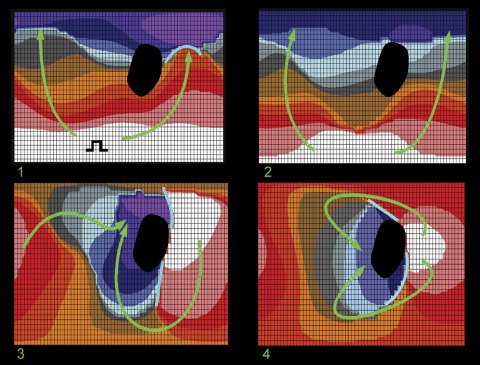
Results: Circuits in which >/=30% of the diastolic pathway (DP) could be defined were identified in 12 VTs (cycle length 357 +/- 60 ms). Eighteen VT episodes were initiated with pacing, and one occurred spontaneously. Ten complete and two partial circuits were mapped (89% +/- 25% of the DP). In all complete circuits, pacing led to the development of unidirectional conduction block at the location of the subsequent VT exit site and the formation of functional block creating a border(s) for subsequent DP. Wavefront velocity in the DP region slowed from 1.22 +/- 0.2 m/s during sinus rhythm to 0.59 +/- 0.14 m/s during VT (P <.005). In 11 initiation episodes, lines of functional block and areas of slow conduction developed progressively over one to six reentrant cycles before a stable DP was established and sustained monomorphic VT ensued. The formation of unidirectional or functional lines of block was not identified during identical pacing protocols that failed to initiate VT (n = 14).
Conclusion: Initiation of sustained monomorphic VT requires the development of unidirectional block and formation of lines of functional block creating borders for a DP in areas of slow conduction. A transitional stage often exists during the initiation process before a stable VT circuit is established.
Figures
Similar articles
-
Mechanism of pacing-induced ventricular fibrillation in the infarcted human heart.Circulation. 2004 Sep 28;110(13):1725-30. doi: 10.1161/01.CIR.0000143043.65045.CF. Epub 2004 Sep 20. Circulation. 2004. PMID: 15381651
-
Radiofrequency catheter ablation of sustained ventricular tachycardia in idiopathic dilated cardiomyopathy.Circulation. 1995 Sep 1;92(5):1159-68. doi: 10.1161/01.cir.92.5.1159. Circulation. 1995. PMID: 7648661
-
Novel mechanism of postinfarction ventricular tachycardia originating in surviving left posterior Purkinje fibers.Heart Rhythm. 2006 Aug;3(8):908-18. doi: 10.1016/j.hrthm.2006.04.019. Epub 2006 Apr 22. Heart Rhythm. 2006. PMID: 16876739
-
Identifying sites for catheter ablation of ventricular tachycardia.Herz. 1992 Jun;17(3):158-70. Herz. 1992. PMID: 1639335 Review.
-
Strategies for catheter ablation of scar-related ventricular tachycardia.Curr Cardiol Rep. 2000 Nov;2(6):537-44. doi: 10.1007/s11886-000-0039-9. Curr Cardiol Rep. 2000. PMID: 11060581 Review.
Cited by
-
The scar: the wind in the perfect storm-insights into the mysterious living tissue originating ventricular arrhythmias.J Interv Card Electrophysiol. 2023 Jan;66(1):27-38. doi: 10.1007/s10840-021-01104-w. Epub 2022 Jan 24. J Interv Card Electrophysiol. 2023. PMID: 35072829 Free PMC article. Review.
-
The Role of Cardiac MRI in the Management of Ventricular Arrhythmias in Ischaemic and Non-ischaemic Dilated Cardiomyopathy.Arrhythm Electrophysiol Rev. 2019 Jul;8(3):191-201. doi: 10.15420/aer.2019.5.1. Arrhythm Electrophysiol Rev. 2019. PMID: 31463057 Free PMC article. Review.
-
Rotational Activation Pattern During Functional Substrate Mapping: Novel Target for Catheter Ablation of Scar-Related Ventricular Tachycardia.Circ Arrhythm Electrophysiol. 2022 Jan;15(1):e010308. doi: 10.1161/CIRCEP.121.010308. Epub 2021 Dec 23. Circ Arrhythm Electrophysiol. 2022. PMID: 34937390 Free PMC article.
-
Techniques for automated local activation time annotation and conduction velocity estimation in cardiac mapping.Comput Biol Med. 2015 Oct 1;65:229-42. doi: 10.1016/j.compbiomed.2015.04.027. Epub 2015 Apr 25. Comput Biol Med. 2015. PMID: 25978869 Free PMC article.
-
Ivabradine: potential clinical applications in critically ill patients.Clin Res Cardiol. 2013 Mar;102(3):171-8. doi: 10.1007/s00392-012-0516-3. Epub 2012 Oct 14. Clin Res Cardiol. 2013. PMID: 23064879 Review.
References
-
- Stevenson W.G., Friedman P.L., Sager P.T. Exploring postinfarction reentrant ventricular tachycardia with entrainment mapping. J Am Coll Cardiol. 1997;29:1180–1189. - PubMed
-
- de Bakker J.M., van Capelle F.J., Janse M.J. Reentry as a cause of ventricular tachycardia in patients with chronic ischemic heart disease: electrophysiologic and anatomic correlation. Circulation. 1988;77:589–606. - PubMed
-
- Downar E., Harris L., Mickleborough L.L., Shaikh N., Parson I.D. Endocardial mapping of ventricular tachycardia in the intact human ventricle: evidence for reentrant mechanisms. J Am Coll Cardiol. 1988;11:783–791. - PubMed
-
- Pogwizd S.M., Hoyt R.H., Saffitz J.E., Corr P.B., Cox J.L., Cain M.E. Reentrant and focal mechanisms underlying ventricular tachycardia in the human heart. Circulation. 1992;86:1872–1887. - PubMed
-
- Roy D., Waxman H.L., Kienzle M.G., Buxton A.E., Marchlinski F.E., Josephson M.E. Clinical characteristics and long-term follow-up in 119 survivors of cardiac arrest: relation to inducibility at electrophysiologic testing. Am J Cardiol. 1983;52:969–974. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
