

Comparison of 30-day outcomes after non-LapBand primary and revisional bariatric surgical procedures from the Longitudinal Assessment of Bariatric Surgery study
- PMID: 20129303
- PMCID: PMC2836857
- DOI: 10.1016/j.soard.2009.10.007
Comparison of 30-day outcomes after non-LapBand primary and revisional bariatric surgical procedures from the Longitudinal Assessment of Bariatric Surgery study
Abstract
Background: The goals were to compare the morbidity and mortality between primary and revisional bariatric surgery and to identify the clinical predictors of adverse outcomes among patients undergoing revisional surgery in the Longitudinal Assessment of Bariatric Surgery consortium. The study was multi-institutional at university hospitals in the United States.
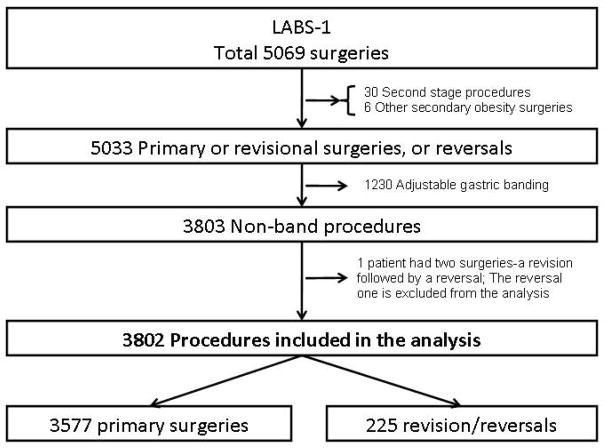
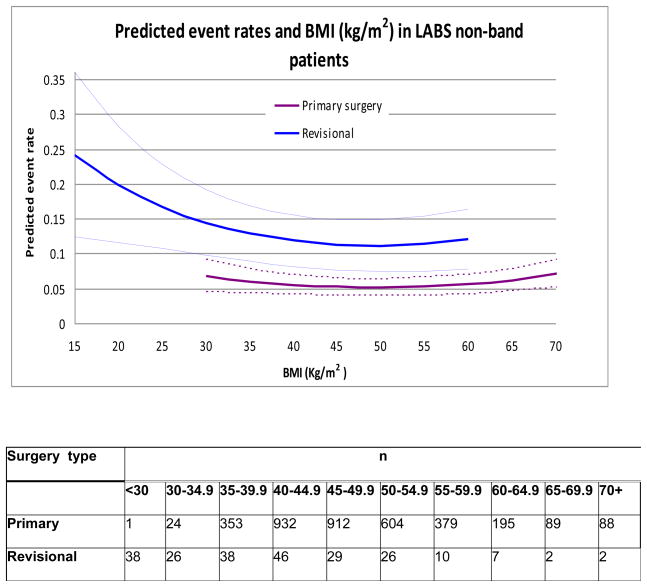
Methods: Data from the LABS-1 (safety) cohort were analyzed, excluding primary gastric banding patients. A total of 3802 LABS-1 patients were included: 3577 who underwent primary surgery and 225 who underwent revisional surgery. The demographic, clinical, operative, and 30-day outcome data were compared between the 2 groups. A nonlinear mixed effects logit model was used to identify independent risk factors for adverse outcomes (death, deep vein thrombosis, pulmonary embolism, reintubation, reoperation, or discharge after 30 days).
Results: Compared with those undergoing revisional surgery, the primary surgery patients were younger (median age 44 versus 49 years, P <.0001) and more likely to be male (20.5% versus 12.7%, P = .006) and heavier (median body mass index 47.3 versus 41.2 kg/m(2), P <.0001) and to have more co-morbidities (P <.0001), including hypertension (56.0% versus 46.0%, P = .0044), diabetes (35.7% versus 20.0%, P <.0001), and sleep apnea (50.3% versus 27.2%, P <.0001). The operative time for the revisional procedures was longer (median 181 versus 135 min, P <.0001) and associated with greater blood loss (median 100 versus <50 mL, P <.0001). Adverse outcomes were more likely after revisional surgery (15.1% versus 5.3%, P <.0001, odds ratio 2.4, 95% confidence interval 1.6-3.6). After adjusting for patient characteristics previously shown to be associated with adverse outcomes, this difference remained statistically significant (odds ratio 2.3, 95% confidence interval 1.5-3.8). The 30-day mortality rate was similar in the 2 groups (.4%).
Conclusion: Revisional surgery was performed without substantial mortality but with a greater incidence of adverse outcomes than was primary bariatric surgery.
2010 American Society for Metabolic and Bariatric Surgery. All rights reserved.
Figures
Comment in
-
Revisional bariatric surgery can be done safely: it's nice to confirm our personal clinical experience with data.Surg Obes Relat Dis. 2010 Mar 4;6(2):223. doi: 10.1016/j.soard.2009.11.010. Epub 2009 Dec 11. Surg Obes Relat Dis. 2010. PMID: 20359672 No abstract available.
Similar articles
-
Characteristics and outcomes for patients undergoing revisional bariatric surgery due to persistent obesity: a retrospective cohort study of 10,589 patients.Surg Endosc. 2023 Jun;37(6):4613-4622. doi: 10.1007/s00464-023-09951-6. Epub 2023 Mar 1. Surg Endosc. 2023. PMID: 36859722
-
Primary Versus Revisional Bariatric and Metabolic Surgery in Patients with a Body Mass Index ≥ 50 kg/m2-90-Day Outcomes and Risk of Perioperative Mortality.Obes Surg. 2024 Aug;34(8):2872-2879. doi: 10.1007/s11695-024-07310-5. Epub 2024 Jun 15. Obes Surg. 2024. PMID: 38879725 Free PMC article.
-
Revisional Malabsorptive Bariatric Surgery: 29-Year Follow-up in a Brazilian Public Hospital.Obes Surg. 2018 Jun;28(6):1504-1510. doi: 10.1007/s11695-017-3023-9. Obes Surg. 2018. PMID: 29159553
-
Revisional Robotic Bariatric Surgery. Largest Single Centre Prospective Cohort Study and Review of the Literature.Chirurgia (Bucur). 2023 Oct;118(5):455-463. doi: 10.21614/chirurgia.2023.v.118.i.5.p.455. Chirurgia (Bucur). 2023. PMID: 37965830 Review.
-
Metabolic outcomes after revisional bariatric surgery: a systematic review and meta-analysis.Surg Obes Relat Dis. 2020 Oct;16(10):1442-1454. doi: 10.1016/j.soard.2020.05.029. Epub 2020 Jun 6. Surg Obes Relat Dis. 2020. PMID: 32711955
Cited by
-
Early post-operative complications: incidence, management, and impact on length of hospital stay. A retrospective comparison between laparoscopic gastric bypass and sleeve gastrectomy.Obes Surg. 2013 Dec;23(12):2004-12. doi: 10.1007/s11695-013-1022-z. Obes Surg. 2013. PMID: 23846474
-
Gastrointestinal Complications After Bariatric Surgery.Gastroenterol Hepatol (N Y). 2015 Aug;11(8):526-35. Gastroenterol Hepatol (N Y). 2015. PMID: 27118949 Free PMC article.
-
Association of Diabetes Mellitus With Postoperative Complications and Mortality After Non-Cardiac Surgery: A Meta-Analysis and Systematic Review.Front Endocrinol (Lausanne). 2022 May 26;13:841256. doi: 10.3389/fendo.2022.841256. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35721703 Free PMC article.
-
Clinical practice guidelines of the European Association for Endoscopic Surgery (EAES) on bariatric surgery: update 2020 endorsed by IFSO-EC, EASO and ESPCOP.Surg Endosc. 2020 Jun;34(6):2332-2358. doi: 10.1007/s00464-020-07555-y. Epub 2020 Apr 23. Surg Endosc. 2020. PMID: 32328827 Free PMC article.
-
Preoperative Detection of Sarcopenic Obesity Helps to Predict the Occurrence of Gastric Leak After Sleeve Gastrectomy.Obes Surg. 2018 Aug;28(8):2379-2385. doi: 10.1007/s11695-018-3169-0. Obes Surg. 2018. PMID: 29500672
References
-
- Ogden CL, Yanovski SZ, Carroll MD, Flegal KM. The epidemiology of obesity. Gastroenterology. 2007;132:2087–102. - PubMed
-
- Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA. 2006;295:1549–55. - PubMed
-
- Nguyen NT, Root J, Zainabadi K, et al. Accelerated growth of bariatric surgery with the introduction of minimally invasive surgery. Arch Surg. 2005;140:1198–202. discussion 203. - PubMed
-
-
http://www.asbs.org/Newsite07/media/asmbs_fs_surgery.pdf .
-
-
- Brolin RE, Cody RP. Weight loss outcome of revisional bariatric operations varies according to the primary procedure. Ann Surg. 2008;248:227–32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
