

Perivenous demyelination: association with clinically defined acute disseminated encephalomyelitis and comparison with pathologically confirmed multiple sclerosis
- PMID: 20129932
- PMCID: PMC2822631
- DOI: 10.1093/brain/awp321
Perivenous demyelination: association with clinically defined acute disseminated encephalomyelitis and comparison with pathologically confirmed multiple sclerosis
Abstract
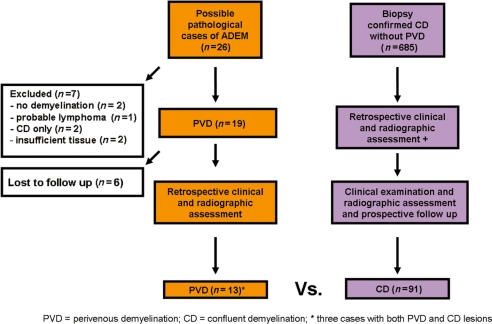
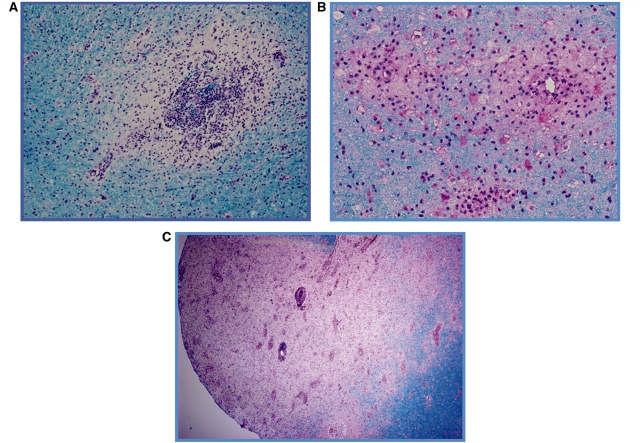
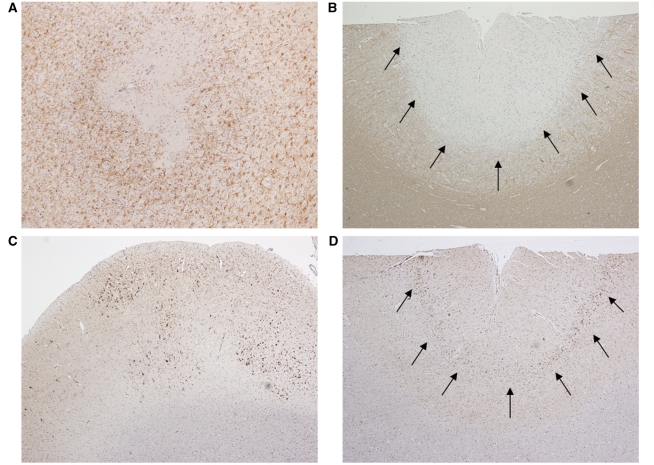
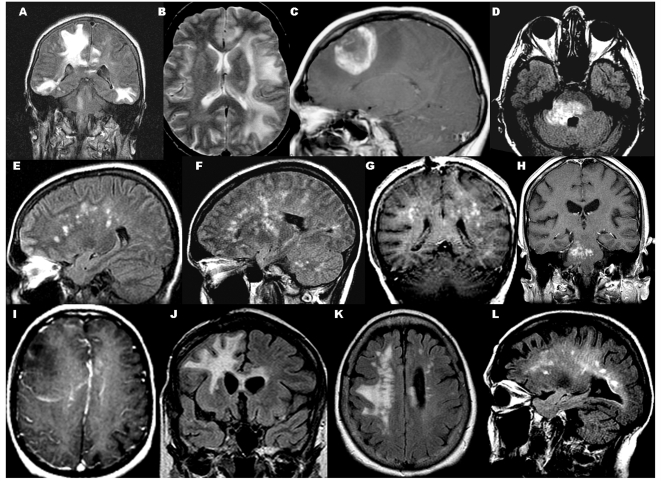
Distinction between acute disseminated encephalomyelitis and acute multiple sclerosis is often clinically difficult. Perivenous demyelination is the pathological hallmark of acute disseminated encephalomyelitis, whereas confluent demyelination is the hallmark of acute multiple sclerosis. We investigated whether perivenous demyelination versus confluent demyelination distinguishes acute disseminated encephalomyelitis from multiple sclerosis. Patients with perivenous demyelination (n = 13; median age 43 years, range 5-67) on brain biopsy and/or autopsy, ascertained retrospectively, were compared with a cohort with confluent demyelination only (n = 91; 84% multiple sclerosis, 16% isolated syndrome at follow-up; median age 39 years, range 10-69). Clinical presentation, course and the International Paediatric Multiple Sclerosis Study Group clinical criteria for acute disseminated encephalomyelitis were assessed in both cohorts. Among the perivenous demyelination cohort, 10 patients had only perivenous demyelination and three also had confluent demyelination. All but one patient with perivenous demyelination only had a monophasic course, whereas two of three with both types had a relapsing course. The perivenous demyelination cohort was more likely than the confluent demyelination cohort to present with encephalopathy (P < 0.001), depressed level of consciousness (P < 0.001), headache (P < 0.001), meningismus (P = 0.04), cerebrospinal fluid pleocytosis (P = 0.04) or multifocal enhancing magnetic resonance imaging lesions (P < 0.001). A distinct pattern of cortical microglial activation and aggregation without associated cortical demyelination was found among six perivenous demyelination patients, all of whom had encephalopathy and four of whom had depressed level of consciousness. This pattern of cortical pathology was not observed in the confluent demyelination cohort, even in one patient with depressed level of consciousness. Clinical criteria were 80% sensitive and 91% specific for pathologically defined acute disseminated encephalomyelitis (perivenous demyelination), but misdiagnosed acute disseminated encephalomyelitis among 9% of patients with confluent demyelination and multiple sclerosis diagnosis at last follow-up. Perivenous demyelination is associated with meningoencephalopathic presentations and a monophasic course. Depressed level of consciousness is a more specific clinical criterion for pathologically confirmed acute disseminated encephalomyelitis than encephalopathy, which over-diagnosed acute disseminated encephalomyelitis among multiple sclerosis patients. A distinct pattern of cortical microglial activation without cortical demyelination may be the pathological correlate of depressed level of consciousness in acute disseminated encephalomyelitis. Although pathological evidence of perivenous demyelination may be superior to clinical criteria for diagnosing acute disseminated encephalomyelitis, the co-occurrence of perivenous and confluent demyelination in some individuals suggests pathogenic overlap between acute disseminated encephalomyelitis and multiple sclerosis and misclassification even with biopsy.
Figures
Similar articles
-
Susceptibility-weighted imaging helps to discriminate pediatric multiple sclerosis from acute disseminated encephalomyelitis.Pediatr Neurol. 2015 Jan;52(1):36-41. doi: 10.1016/j.pediatrneurol.2014.10.014. Epub 2014 Oct 16. Pediatr Neurol. 2015. PMID: 25532777 Free PMC article.
-
Acute disseminated encephalomyelitis, multiphasic disseminated encephalomyelitis and multiple sclerosis in children.Brain. 2000 Dec;123 Pt 12:2407-22. doi: 10.1093/brain/123.12.2407. Brain. 2000. PMID: 11099444 Clinical Trial.
-
Myelin oligodendrocyte glycoprotein antibody-associated disease: an immunopathological study.Brain. 2020 May 1;143(5):1431-1446. doi: 10.1093/brain/awaa102. Brain. 2020. PMID: 32412053
-
Pediatric central nervous system inflammatory demyelination: acute disseminated encephalomyelitis, clinically isolated syndromes, neuromyelitis optica, and multiple sclerosis.Curr Opin Neurol. 2009 Jun;22(3):233-40. doi: 10.1097/wco.0b013e32832b4c47. Curr Opin Neurol. 2009. PMID: 19434783 Review.
-
Acute disseminated encephalomyelitis.J Child Neurol. 2012 Nov;27(11):1408-25. doi: 10.1177/0883073812455104. Epub 2012 Aug 21. J Child Neurol. 2012. PMID: 22914374 Review.
Cited by
-
Venous hemodynamics in neurological disorders: an analytical review with hydrodynamic analysis.BMC Med. 2013 May 31;11:142. doi: 10.1186/1741-7015-11-142. BMC Med. 2013. PMID: 23724917 Free PMC article. Review.
-
Three Types of Demyelination, Perivenous, Confluent, and Perineuronal Nets-Rich in a COVID-19 Patient With Meningoencephalomyelitis.Cureus. 2023 Dec 24;15(12):e51049. doi: 10.7759/cureus.51049. eCollection 2023 Dec. Cureus. 2023. PMID: 38269235 Free PMC article.
-
Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disorders: Toward a New Spectrum of Inflammatory Demyelinating CNS Disorders?Front Immunol. 2018 Nov 29;9:2753. doi: 10.3389/fimmu.2018.02753. eCollection 2018. Front Immunol. 2018. PMID: 30555462 Free PMC article. Review.
-
Acute disseminated encephalomyelitis (ADEM)-like illness in a pediatric patient following COVID-19 vaccination.BJR Case Rep. 2023 Feb 20;9(2):20220097. doi: 10.1259/bjrcr.20220097. eCollection 2023 Mar. BJR Case Rep. 2023. PMID: 36998331 Free PMC article.
-
Gender and Age Differences in Seronegative Pediatric Acute Disseminated Encephalomyelitis Profiles: Results and Insights from a Tertiary Center.Iran J Child Neurol. 2025;19(2):77-91. doi: 10.22037/ijcn.v19i2.46613. Epub 2025 Mar 11. Iran J Child Neurol. 2025. PMID: 40231275 Free PMC article.
References
-
- Brinar VV, Poser CM. The spectrum of disseminated encephalomyelitis. Clin Neurol Neurosurg. 2006;108:295–310. - PubMed
-
- Callen DJ, Shroff MM, Branson HM, Li DK, Lotze T, Stephens D, et al. Role of MRI in the differentiation of ADEM from MS in children. Neurology. 2008;72:968–73. - PubMed
-
- Cohen O, Steiner-Birmanns B, Biran I, Abramsky O, Honigman S, Steiner I. Recurrence of acute disseminated encephalomyelitis at the previously affected brain site. Arch Neurol. 2001;58:797–801. - PubMed
-
- Dagher AP, Smirniotopoulos J. Tumefactive demyelinating lesions. Neuroradiology. 1996;38:560–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
