

Wake-up stroke: clinical and neuroimaging characteristics
- PMID: 20130399
- PMCID: PMC2914433
- DOI: 10.1159/000278929
Wake-up stroke: clinical and neuroimaging characteristics
Abstract
Background: Approximately 25% of ischemic stroke patients awaken with neurological deficits. In these patients, in whom the time from symptom onset is uncertain, brain imaging is a potential strategy to characterize the ischemia duration and the presence of salvageable brain tissue.
Methods: We prospectively evaluated consecutive patients with acute ischemic stroke. CT angiography and CT perfusion (CTP) were performed in patients within 24 h of symptom onset. The patients were classified into 'known onset', 'indefinite onset but not on awakening' and 'wake-up stroke' groups.
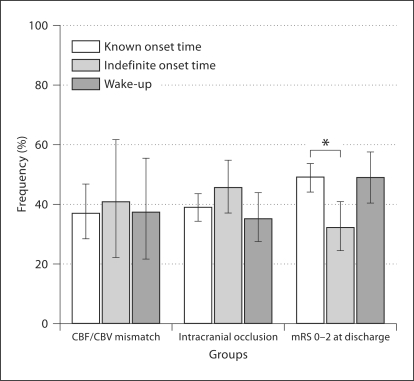
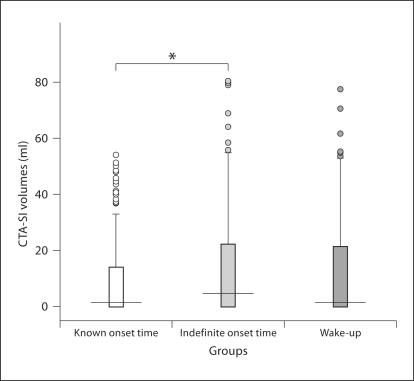
Results: Of 676 patients evaluated, 420 had known-onset strokes, 131 wake-up strokes and 125 strokes with an indefinite time of symptom onset. Ischemic lesion volumes were higher in patients with indefinite-onset strokes (p = 0.04). The frequencies of CTP mismatch and of large-vessel intracranial occlusions were similar among the groups (p = 0.9 and p = 0.2, respectively).
Conclusion: The considerable prevalence of CTP mismatch and of intracranial artery occlusions in our patients with wake-up strokes suggests that arterial and perfusion imaging might be particularly important in this population. Revised indications for thrombolysis by using imaging-based protocols might offer these patients the prospect of receiving acute stroke treatment even without a clear time of symptom onset.
(c) 2010 S. Karger AG, Basel.
Figures
References
-
- Nadeau JO, Fang J, Kapral MK, Silver FL, Hill MD. Outcome after stroke upon awakening. Can J Neurol Sci. 2005;32:232–236. - PubMed
-
- National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333:1581–1587. - PubMed
-
- Adams HPJ, Leira EC, Torner JC, Barnathan E, Padgett L, Effron MB, Hacke W. Treating patients with ‘wake-up’ stroke: the experience of the AbESTT-II trial. Stroke. 2008;39:3277–3282. - PubMed
-
- Fink JN, Kumar S, Horkan C, Linfante I, Selim MH, Caplan LR, Schlaug G. The stroke patient who woke up: clinical and radiological features, including diffusion and perfusion MRI. Stroke. 2002;33:988–993. - PubMed
