

Effects of mild hypothermia on hemodynamics in cardiac arrest survivors and isolated failing human myocardium
- PMID: 20130890
- PMCID: PMC2858797
- DOI: 10.1007/s00392-010-0113-2
Effects of mild hypothermia on hemodynamics in cardiac arrest survivors and isolated failing human myocardium
Abstract
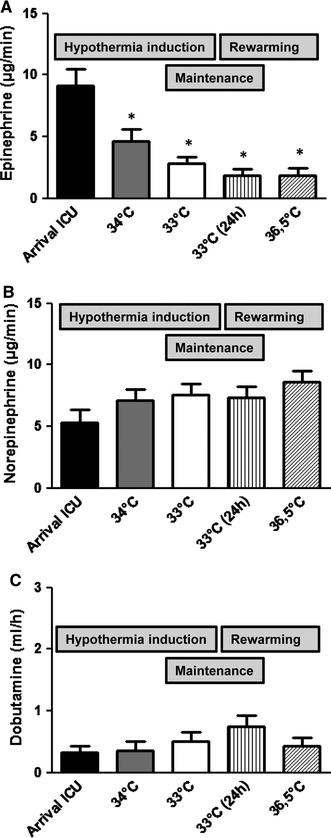
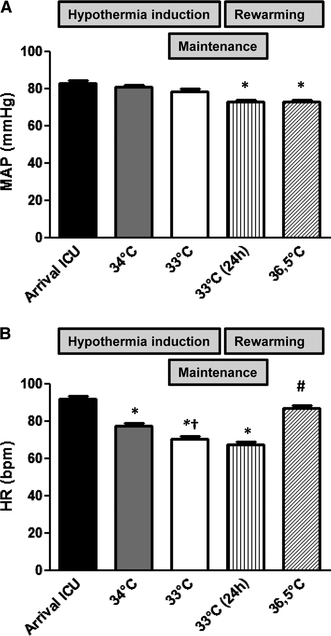
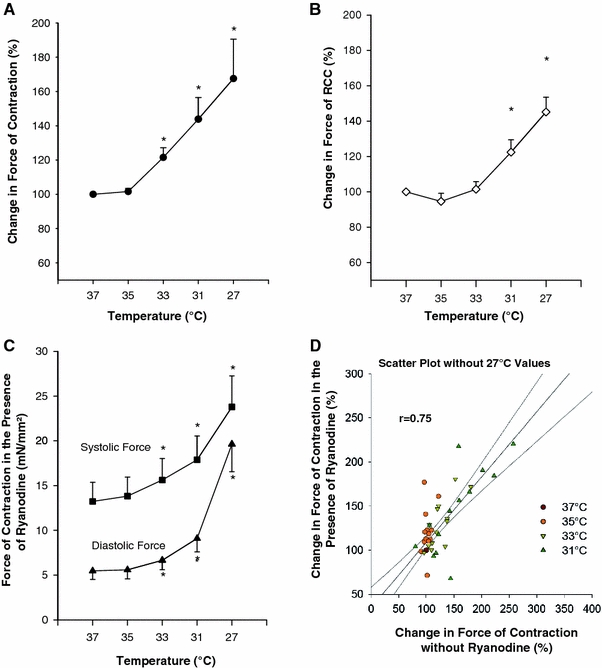
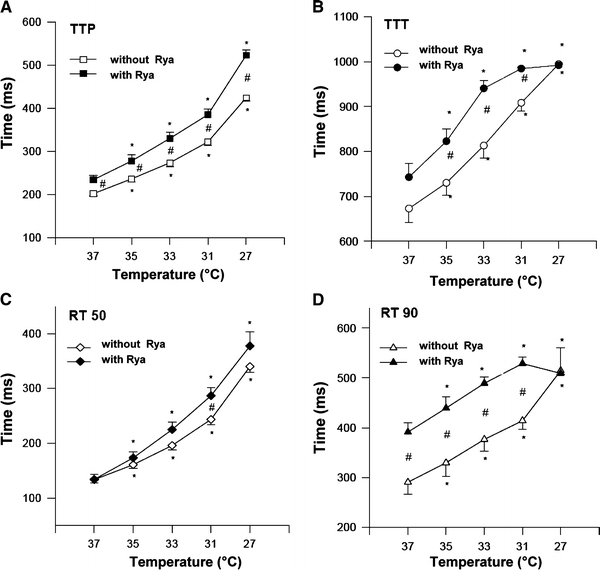
Post-cardiac arrest myocardial dysfunction is a common phenomenon after return of spontaneous circulation (ROSC) and contributes to hemodynamic instability and low survival rates after cardiac arrest. Mild hypothermia for 24 h after ROSC has been shown to significantly improve neurologic recovery and survival rates. In the present study we investigate the influence of therapeutic hypothermia on hemodynamic parameters in resuscitated patients and on contractility in failing human myocardium. We analyzed hemodynamic data from 200 cardiac arrest survivors during the hypothermia period. The initial LVEF was 32.6 +/- 1.2% indicating a significantly impaired LV function. During hypothermia induction, the infusion rate of epinephrine could be significantly reduced from 9.1 +/- 1.3 microg/min [arrival intensive care unit (ICU) 35.4 degrees C] to 4.6 +/- 1.0 microg/min (34 degrees C) and 2.8 +/- 0.5 microg/min (33 degrees C). The dobutamine and norepinephrine application rates were not changed significantly. The mean arterial blood pressure remained stable. The mean heart rate significantly decreased from 91.8 +/- 1.7 bpm (arrival ICU) to 77.3 +/- 1.5 bpm (34 degrees C) and 70.3 +/- 1.4 bpm (33 degrees C). In vitro we investigated the effect of hypothermia on isolated ventricular muscle strips from explanted failing human hearts. With decreasing temperature, the contractility increased to a maximum of 168 +/- 23% at 27 degrees C (n = 16, P < 0.05). Positive inotropic response to hypothermia was accompanied by moderately increased rapid cooling contractures as a measure of sarcoplasmic reticulum (SR) Ca(2+) content, but can be elicited even when the SR Ca(2+) release is blocked in the presence of ryanodine. Contraction and relaxation kinetics are prolonged with hypothermia, indicating increased Ca(2+) sensitivity as the main mechanism responsible for inotropy. In conclusion, mild hypothermia stabilizes hemodynamics in cardiac arrest survivors which might contribute to improved survival rates in these patients. Mechanistically, we demonstrate that hypothermia improves contractility in failing human myocardium most likely by increasing Ca(2+)-sensitivity.
Figures
Similar articles
-
Inotropic Effects of Experimental Hyperthermia and Hypothermia on Left Ventricular Function in Pigs-Comparison With Dobutamine.Crit Care Med. 2016 Mar;44(3):e158-67. doi: 10.1097/CCM.0000000000001358. Crit Care Med. 2016. PMID: 26474110
-
Influence of mild hypothermia on myocardial contractility and circulatory function.Basic Res Cardiol. 2001 Apr;96(2):198-205. doi: 10.1007/s003950170071. Basic Res Cardiol. 2001. PMID: 11327339
-
[Effect of pre-arrest and post-arrest mild hypothermia on myocardial function of ventricular fibrillation after restoration of spontaneous circulation in rabbits].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2015 Mar;27(3):185-9. doi: 10.3760/cma.j.issn.2095-4352.2015.03.006. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2015. PMID: 25757967 Chinese.
-
Impact of hypothermia on cardiac performance during targeted temperature management after cardiac arrest.Resuscitation. 2019 Sep;142:1-7. doi: 10.1016/j.resuscitation.2019.06.276. Epub 2019 Jun 22. Resuscitation. 2019. PMID: 31238037
-
Effects of temperature control on hyperthermia-related cardiac dysfunction in a porcine model of cardiac arrest.Cryobiology. 2023 Mar;110:49-55. doi: 10.1016/j.cryobiol.2022.12.017. Epub 2022 Dec 9. Cryobiology. 2023. PMID: 36509162
Cited by
-
The Modified Glasgow Outcome Score for the prediction of outcome in patients after cardiac arrest: a prospective clinical proof of concept study.Clin Res Cardiol. 2012 Jul;101(7):533-43. doi: 10.1007/s00392-012-0423-7. Epub 2012 Feb 10. Clin Res Cardiol. 2012. PMID: 22322567
-
Influence of algorithm-based analgesia and sedation in patients after sudden cardiac arrest.Clin Res Cardiol. 2012 Mar;101(3):175-83. doi: 10.1007/s00392-011-0378-0. Epub 2011 Nov 3. Clin Res Cardiol. 2012. PMID: 22048697 Clinical Trial.
-
Effects of Mild Therapeutic Hypothermia on Hemodynamic Support in Cardiogenic Shock After Acute Myocardial Infarction.Cureus. 2025 Jun 20;17(6):e86407. doi: 10.7759/cureus.86407. eCollection 2025 Jun. Cureus. 2025. PMID: 40688950 Free PMC article.
-
Successful Re-Initiation of Therapeutic Hypothermia as Adjunctive Salvage Therapy in a Case of Refractory Cardiogenic Shock Due to Acute Myocardial Infarction.Am J Case Rep. 2019 Mar 12;20:323-329. doi: 10.12659/AJCR.913459. Am J Case Rep. 2019. PMID: 30858348 Free PMC article.
-
Feasibility and beneficial effects of an early goal directed therapy after cardiac arrest: evaluation by conductance method.Sci Rep. 2021 Mar 5;11(1):5326. doi: 10.1038/s41598-021-83925-3. Sci Rep. 2021. PMID: 33674623 Free PMC article.
References
-
- Nadkarni VM, Larkin GL, Peberdy MA, Carey SM, Kaye W, Mancini ME, Nichol G, Lane-Truitt T, Potts J, Ornato JP, Berg RA, for the National Registry of Cardiopulmonary Resuscitation Investigators First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults. JAMA. 2006;295:50–57. doi: 10.1001/jama.295.1.50. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
