

Distinguishing SWEDDs patients with asymmetric resting tremor from Parkinson's disease: a clinical and electrophysiological study
- PMID: 20131394
- PMCID: PMC2996567
- DOI: 10.1002/mds.23019
Distinguishing SWEDDs patients with asymmetric resting tremor from Parkinson's disease: a clinical and electrophysiological study
Abstract
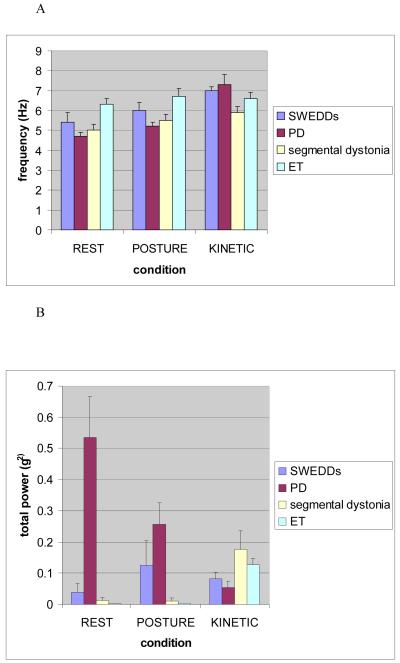
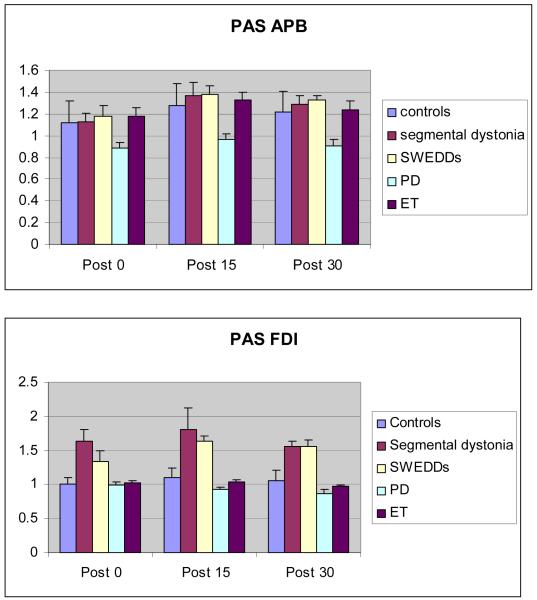
Approximately 10% of patients diagnosed clinically with early Parkinson's disease (PD) have normal dopaminergic functional imaging (Scans Without Evidence of Dopaminergic Deficit [SWEDDs]). An important subgroup of SWEDDs are those with asymmetric rest tremor resembling parkinsonian tremor. Clinical and pathophysiological features which could help to distinguish SWEDDs from PD have not been explored. We therefore studied clinical details including non-motor symptoms in 25 tremulous SWEDDs patients in comparison to 25 tremor-dominant PD patients. Blinded video rating was used to compare examination findings. Electrophysiological tremor parameters and also response to a cortical plasticity protocol using paired associative stimulation (PAS) was studied in 9 patients with SWEDDs, 9 with tremor-dominant PD (with abnormal dopamine transporter single photon emission computed tomography findings), 8 with segmental dystonia, and 8 with essential tremor (ET). Despite clinical overlap, lack of true bradykinesia, presence of dystonia, and head tremor favored a diagnosis of SWEDDs, whereas re-emergent tremor, true fatiguing or decrement, good response to dopaminergic drugs, and presence of non-motor symptoms favored PD. A single tremor parameter could not differentiate between groups, but the combination of re-emergent tremor and highest tremor amplitude at rest was characteristic of PD tremor. SWEDDs and segmental dystonia patients exhibited an abnormal exaggerated response to the PAS protocol, in contrast to a subnormal response in PD and a normal response in ET. We conclude that despite clinical overlap, there are features that can help to distinguish between PD and SWEDDs which may be useful in clinical practice. The underlying pathophysiology of SWEDDs differs from PD but has similarities with primary dystonia.
(c) 2010 Movement Disorder Society.
Figures
Comment in
-
Distinguishing scan without evidence of dopaminergic depletion patients with asymmetric resting tremor from Parkinson's disease: a clinical diagnosis of dystonia is required.Mov Disord. 2010 Dec 15;25(16):2899. doi: 10.1002/mds.23390. Mov Disord. 2010. PMID: 20925066 No abstract available.
References
-
- Bain PG, Findley LJ, Britton TC, Rothwell JC, Gresty MA, Thompson PD, et al. Primary writing tremor. Brain. 1995;118(Pt 6):1461–72. - PubMed
-
- Bain PG, Findley LJ, Thompson PD, Gresty MA, Rothwell JC, Harding AE, et al. A study of hereditary essential tremor. Brain. 1994;117(Pt 4):805–24. - PubMed
-
- Chaudhuri KR, Healy DG, Schapira AH. Non-motor symptoms of Parkinson’s disease: diagnosis and management. Lancet Neurol. 2006;5:235–45. - PubMed
-
- Chaudhuri KR, Martinez-Martin P, Schapira AH, Stocchi F, Sethi K, Odin P, et al. International multicenter pilot study of the first comprehensive self-completed nonmotor symptoms questionnaire for Parkinson’s disease: the NMSQuest study. Mov Disord. 2006;21:916–23. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
