

CyberKnife radiosurgery for inoperable stage IA non-small cell lung cancer: 18F-fluorodeoxyglucose positron emission tomography/computed tomography serial tumor response assessment
- PMID: 20132557
- PMCID: PMC2830958
- DOI: 10.1186/1756-8722-3-6
CyberKnife radiosurgery for inoperable stage IA non-small cell lung cancer: 18F-fluorodeoxyglucose positron emission tomography/computed tomography serial tumor response assessment
Abstract
Objective: To report serial 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography (PET)/computed tomography (CT) tumor response following CyberKnife radiosurgery for stage IA non-small cell lung cancer (NSCLC).
Methods: Patients with biopsy-proven inoperable stage IA NSCLC were enrolled into this IRB-approved study. Targeting was based on 3-5 gold fiducial markers implanted in or near tumors. Gross tumor volumes (GTVs) were contoured using lung windows; margins were expanded by 5 mm to establish the planning treatment volumes (PTVs). Doses ranged from 42-60 Gy in 3 equal fractions. 18F-FDG PET/CT was performed prior to and at 3-6-month, 9-15 months and 18-24 months following treatment. The tumor maximum standardized uptake value (SUV(max)) was recorded for each time point.
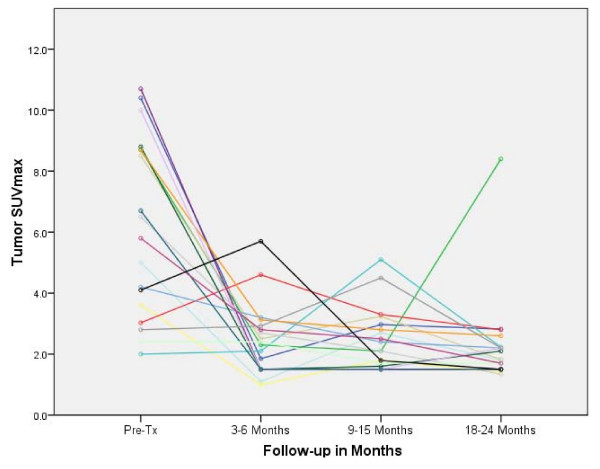
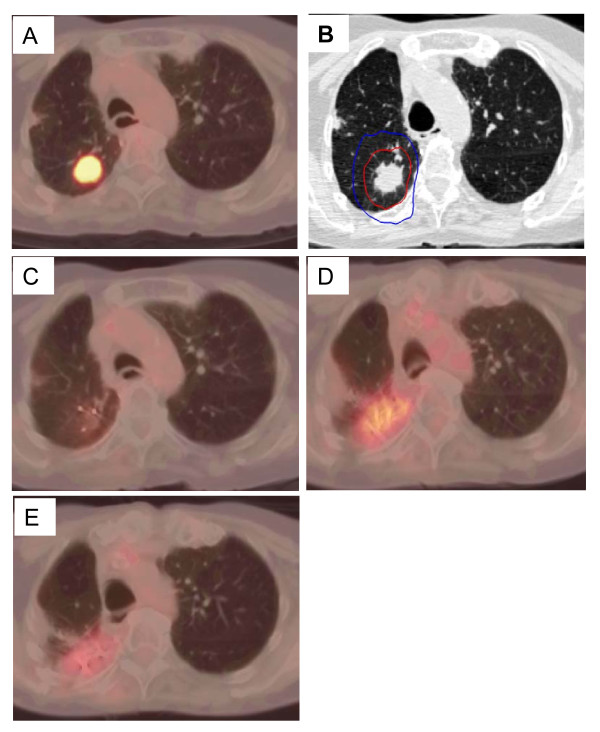
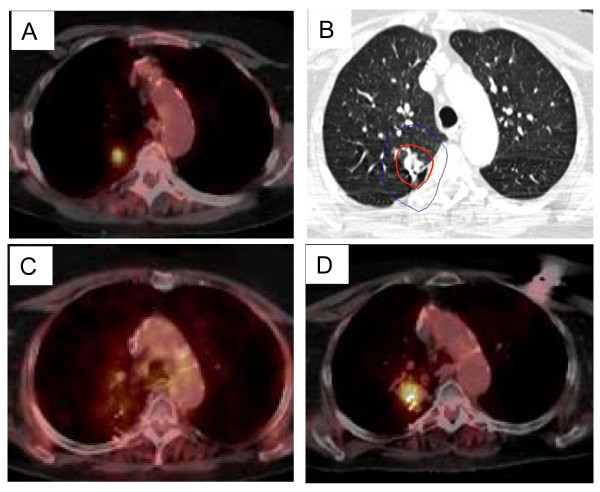
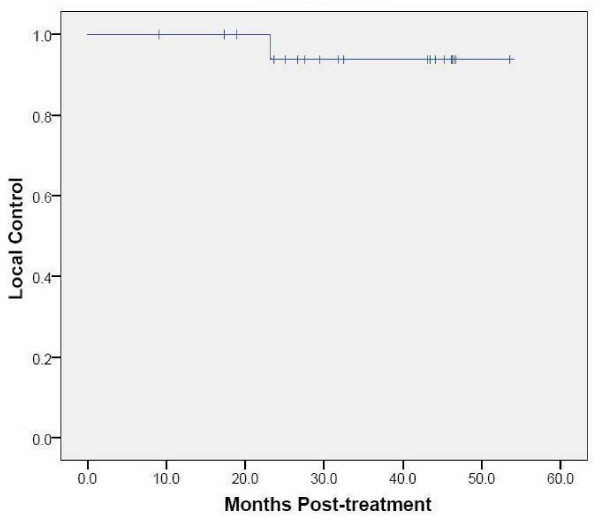
Results: Twenty patients with an average maximum tumor diameter of 2.2 cm were treated over a 3-year period. A mean dose of 51 Gy was delivered to the PTV in 3 to 11 days (mean, 7 days). The 30-Gy isodose contour extended an average of 2 cm from the GTV. At a median follow-up of 43 months, the 2-year Kaplan-Meier overall survival estimate was 90% and the local control estimate was 95%. Mean tumor SUV(max) before treatment was 6.2 (range, 2.0 to 10.7). During early follow-up the mean tumor SUV(max) remained at 2.3 (range, 1.0 to 5.7), despite transient elevations in individual tumor SUV(max) levels attributed to peritumoral radiation-induced pneumonitis visible on CT imaging. At 18-24 months the mean tumor SUV(max) for controlled tumors was 2.0, with a narrow range of values (range, 1.5 to 2.8). A single local failure was confirmed at 24 months in a patient with an elevated tumor SUV(max) of 8.4.
Conclusion: Local control and survival following CyberKnife radiosurgery for stage IA NSCLC is exceptional. Early transient increases in tumor SUV(max) are likely related to radiation-induced pneumonitis. Tumor SUV(max) values return to background levels at 18-24 months, enhancing 18F-FDG PET/CT detection of local failure. The value of 18F-FDG PET/CT imaging for surveillance following lung SBRT deserves further study.
Figures


Similar articles
-
A pilot trial of serial 18F-fluorodeoxyglucose positron emission tomography in patients with medically inoperable stage I non-small-cell lung cancer treated with hypofractionated stereotactic body radiotherapy.Int J Radiat Oncol Biol Phys. 2010 Mar 1;76(3):789-95. doi: 10.1016/j.ijrobp.2009.02.051. Epub 2009 May 25. Int J Radiat Oncol Biol Phys. 2010. PMID: 19473777 Free PMC article. Clinical Trial.
-
Residual ¹⁸F-FDG-PET uptake 12 weeks after stereotactic ablative radiotherapy for stage I non-small-cell lung cancer predicts local control.Int J Radiat Oncol Biol Phys. 2012 Jul 15;83(4):e551-5. doi: 10.1016/j.ijrobp.2012.01.012. Epub 2012 Mar 13. Int J Radiat Oncol Biol Phys. 2012. PMID: 22417800
-
Maximum standardized uptake value from staging FDG-PET/CT does not predict treatment outcome for early-stage non-small-cell lung cancer treated with stereotactic body radiotherapy.Int J Radiat Oncol Biol Phys. 2010 Nov 15;78(4):1033-9. doi: 10.1016/j.ijrobp.2009.09.081. Epub 2010 May 14. Int J Radiat Oncol Biol Phys. 2010. PMID: 20472359
-
Primary tumor standardized uptake value measured on F18-Fluorodeoxyglucose positron emission tomography is of prediction value for survival and local control in non-small-cell lung cancer receiving radiotherapy: meta-analysis.J Thorac Oncol. 2014 Jun;9(6):834-42. doi: 10.1097/JTO.0000000000000185. J Thorac Oncol. 2014. PMID: 24787963 Free PMC article. Review.
-
Risk-adapted robotic stereotactic body radiation therapy for inoperable early-stage non-small-cell lung cancer.Strahlenther Onkol. 2018 Feb;194(2):91-97. doi: 10.1007/s00066-017-1194-x. Epub 2017 Aug 15. Strahlenther Onkol. 2018. PMID: 28812120 Review. English.
Cited by
-
Local Recurrence Risk Score to Predict Relapse after Stereotactic Body Radiation Therapy for Lung Tumors.J Clin Med. 2022 Oct 31;11(21):6445. doi: 10.3390/jcm11216445. J Clin Med. 2022. PMID: 36362674 Free PMC article.
-
Early PET-CT After Stereotactic Radiotherapy for Stage 1 Non-small Cell Lung Carcinoma Is Predictive of Local Control.In Vivo. 2018 Jan-Feb;32(1):121-124. doi: 10.21873/invivo.11213. In Vivo. 2018. PMID: 29275308 Free PMC article.
-
Stereotactic body radiation therapy for stage I non-small cell lung cancer: a small academic hospital experience.Front Oncol. 2014 Oct 20;4:287. doi: 10.3389/fonc.2014.00287. eCollection 2014. Front Oncol. 2014. PMID: 25368843 Free PMC article.
-
CyberKnife with Tumor Tracking: An Effective Treatment for High-Risk Surgical Patients with Single Peripheral Lung Metastases.Front Oncol. 2012 Jun 29;2:63. doi: 10.3389/fonc.2012.00063. eCollection 2012. Front Oncol. 2012. PMID: 22754870 Free PMC article.
-
Evaluation of the influence of tumor location and size on the difference of dose calculation between Ray Tracing algorithm and Fast Monte Carlo algorithm in stereotactic body radiotherapy of non-small cell lung cancer using CyberKnife.J Appl Clin Med Phys. 2013 Sep 6;14(5):68-78. doi: 10.1120/jacmp.v14i5.4280. J Appl Clin Med Phys. 2013. PMID: 24036860 Free PMC article.
References
-
- Uematsu M, Shioda A, Suda A. Computed tomography-guided frameless stereotactic radiotherapy for stage I non-small cell lung cancer: a 5-year experience. Int J Radiat Oncol Biol Phys. 2001;51:666–670. - PubMed
-
- Onishi H, Araki T, Shirato H, Nagata Y, Hiraoka M, Gomi K, Yamashita T, Niibe Y, Karasawa K, Hayakawa K, Takai Y, Kimura T, Hirokawa Y, Takeda A, Ouchi A, Hareyama M, Kokubo M, Hara R, Itami J, Yamada K. Stereotactic hypofractionated high-dose irradiation for stage I nonsmall cell lung carcinoma: clinical outcomes in 245 subjects in a Japanese multiinstitutional study. Cancer. 2004;101:1623–1631. doi: 10.1002/cncr.20539. - DOI - PubMed
-
- McGarry RC, Papiez L, Williams M. Stereotactic body radiation therapy of early-stage non-small-cell lung carcinoma: phase I study. Int J Radiat Oncol Biol Phys. 2005;63:1010–1015. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
