

Sustaining reductions in catheter related bloodstream infections in Michigan intensive care units: observational study
- PMID: 20133365
- PMCID: PMC2816728
- DOI: 10.1136/bmj.c309
Sustaining reductions in catheter related bloodstream infections in Michigan intensive care units: observational study
Abstract
Objectives: To evaluate the extent to which intensive care units participating in the initial Keystone ICU project sustained reductions in rates of catheter related bloodstream infections. Design Collaborative cohort study to implement and evaluate interventions to improve patients' safety.
Setting: Intensive care units predominantly in Michigan, USA.
Intervention: Conceptual model aimed at improving clinicians' use of five evidence based recommendations to reduce rates of catheter related bloodstream infections rates, with measurement and feedback of infection rates. During the sustainability period, intensive care unit teams were instructed to integrate this intervention into staff orientation, collect monthly data from hospital infection control staff, and report infection rates to appropriate stakeholders.
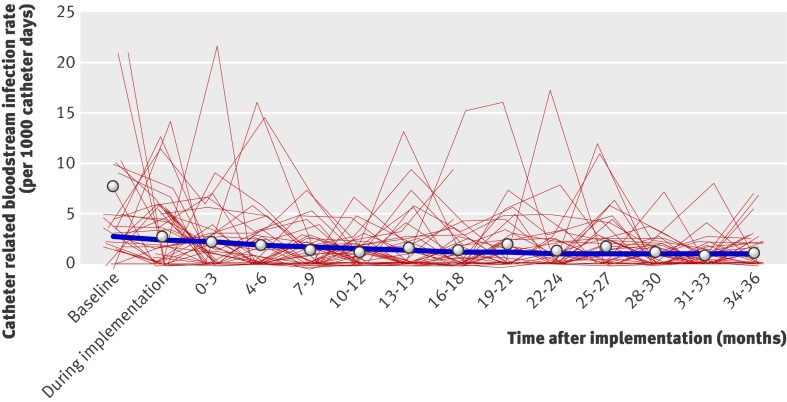
Main outcome measures: Quarterly rate of catheter related bloodstream infections per 1000 catheter days during the sustainability period (19-36 months after implementation of the intervention).
Results: Ninety (87%) of the original 103 intensive care units participated, reporting 1532 intensive care unit months of data and 300 310 catheter days during the sustainability period. The mean and median rates of catheter related bloodstream infection decreased from 7.7 and 2.7 (interquartile range 0.6-4.8) at baseline to 1.3 and 0 (0-2.4) at 16-18 months and to 1.1 and 0 (0.0-1.2) at 34-36 months post-implementation. Multilevel regression analysis showed that incidence rate ratios decreased from 0.68 (95% confidence interval 0.53 to 0.88) at 0-3 months to 0.38 (0.26 to 0.56) at 16-18 months and 0.34 (0.24-0.48) at 34-36 months post-implementation. During the sustainability period, the mean bloodstream infection rate did not significantly change from the initial 18 month post-implementation period (-1%, 95% confidence interval -9% to 7%).
Conclusions: The reduced rates of catheter related bloodstream infection achieved in the initial 18 month post-implementation period were sustained for an additional 18 months as participating intensive care units integrated the intervention into practice. Broad use of this intervention with achievement of similar results could substantially reduce the morbidity and costs associated with catheter related bloodstream infections.
Conflict of interest statement
Competing interests: PJP and CAG received grant support from the Agency for Healthcare Research and Quality, the Robert Wood Johnson Foundation, the National Patient Safety Agency, and the World Health Organization to study and improve quality of care, including catheter related bloodstream infections. They have received lecture fees from various healthcare organisations, and CAG has also received lecture fees from government agencies to speak on quality and patient safety. SC has grant support from Cubist and Astellas, has served as a consultant for Merck, and has been on the advisory boards for Astellas, Forrest, and Cadence. JBS and JAM have grant support from the Robert Wood Johnson Foundation. PP has received lecture fees from Lilly, Merck, Edward Life Sciences, and Sage for various speaking engagements. DMN has had grant and contract support from the National Institutes of Health/National Heart Lung and Blood Institute and a clinician-scientists award from the Canadian Institutes of Health Research.
Figures
References
-
- Burke JP. Infection control—a problem for patient safety. N Engl J Med 2003;348:651-6. - PubMed
-
- Mermel LA. Prevention of intravascular catheter-related infections. Ann Intern Med 2000;132:391-402. - PubMed
-
- O’Grady NP, Alexander M, Dellinger EP, Gerberding JL, Heard SO, Maki DG, et al. Guidelines for the prevention of intravascular catheter-related infections. MMWR 2002;55:1-26. - PubMed
-
- Pronovost P, Needham D, Berenholtz S, Sinopoli D, Chu H, Cosgrove S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med 2006;355:2725-32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical