

Undiagnosed diabetes in kidney transplant candidates: a case-finding strategy
- PMID: 20133490
- PMCID: PMC2849698
- DOI: 10.2215/CJN.07501009
Undiagnosed diabetes in kidney transplant candidates: a case-finding strategy
Abstract
Background and objectives: Guidelines recommend that candidates for kidney transplantation (KTx) who do not have diabetes perform a pretransplantation oral glucose tolerance test (OGTT) when fasting plasma glucose (FPG) is <110 mg/dl (<6.1 mmol/L); however, the OGTT is potentially costly and cumbersome. We studied the role of the OGTT for diagnosing diabetes and the accuracy of FPG and glycated hemoglobin (HbA(1c)) for predicting a diabetic OGTT before KTx.
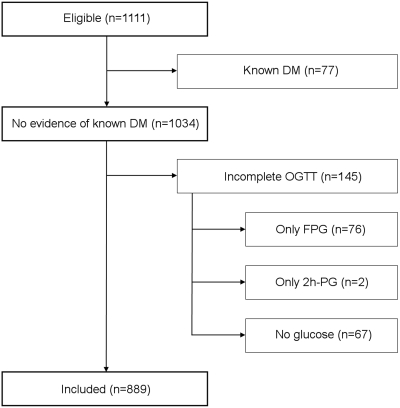
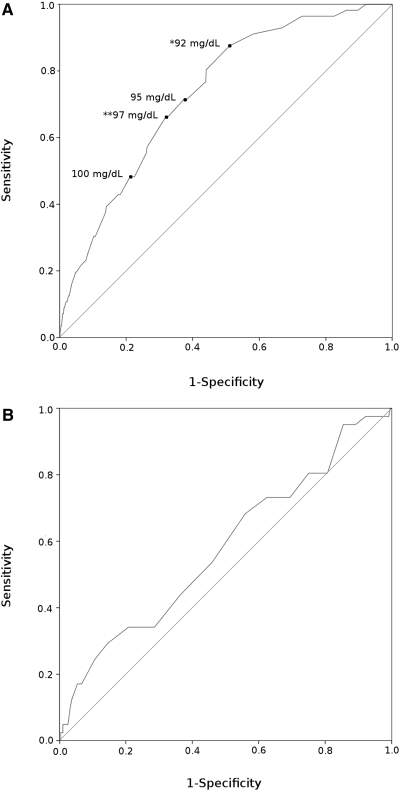
Design, setting, participants, & measurements: In this cross-sectional study, 889 first single-kidney transplant candidates without diabetes, mainly white, performed an OGTT during the transplantation workup. Results were studied using receiver operating characteristic analysis.
Results: Of 72 (8.1%) patients with undiagnosed diabetes, only 16 (22%) had a diabetic FPG (> or =126 mg/dl [> or =7.0 mmol/L]). In patients with a nondiabetic FPG, diabetes (2-hour plasma glucose [2h-PG] > or =200 mg/dl [> or =11.1 mmol/L]) was predicted by FPG but not by HbA(1c). Performing the OGTT in patients with FPG 92 to 125 mg/dl (5.1 to 6.9 mmol/L) identified 65 (90%) patients with diabetes (16 by FPG, 49 by 2h-PG) and required seven OGTTs per patient identified. Subjecting all patients with FPG <110 mg/dl (<6.1 mmol/L) to the OGTT identified 60 (83%) patients with diabetes (16 by FPG, 44 by 2h-PG) but required 14 OGTTs per patient.
Conclusions: The OGTT was paramount in finding most cases of undiagnosed diabetes before KTx. FPG but not HbA(1c) predicted a diabetic OGTT. We suggest that white KTx candidates without diabetes perform a pretransplantation OGTT when FPG is 92 to 125 mg/dl (5.1 to 6.9 mmol/L).
Figures
References
-
- Vincenti F, Friman S, Scheuermann E, Rostaing L, Jenssen T, Campistol JM, Uchida K, Pescovitz MD, Marchetti P, Tuncer M, Citterio F, Wiecek A, Chadban S, El-Shahawy M, Budde O, Goto N: Results of an international, randomized trial comparing glucose metabolism disorders and outcome with cyclosporine versus tacrolimus. Am J Transplant 7: 1506–1514, 2007 - PubMed
-
- Lin-Tan DT, Lin JL, Wang LH, Wang LM, Huang LM, Liu L, Huang JY, Huang YL: Fasting glucose levels in predicting 1-year all-cause mortality in patients who do not have diabetes and are on maintenance hemodialysis. J Am Soc Nephrol 18: 2385–2391, 2007 - PubMed
-
- Mathew JT, Rao M, Job V, Ratnaswamy S, Jacob CK: Post-transplant hyperglycaemia: A study of risk factors. Nephrol Dial Transplant 18: 164–171, 2003 - PubMed
-
- Nam JH, Mun JI, Kim SI, Kang SW, Choi KH, Park K, Ahn CW, Cha BS, Song YD, Lim SK, Kim KR, Lee HC, Huh KB: Beta-cell dysfunction rather than insulin resistance is the main contributing factor for the development of postrenal transplantation diabetes mellitus. Transplantation 71: 1417–1423, 2001 - PubMed
-
- Ramesh Prasad GV, Huang M, Bandukwala F, Nash MM, Rapi L, Montada-Atin T, Meliton G, Zaltzman JS: Pre-transplantation glucose testing for predicting new-onset diabetes mellitus after renal transplantation. Clin Nephrol 71: 140–146, 2009 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
